Mechanical Reperfusion of Subocclusive Plaque Erosion: 30-Month Outcome of an Optical Coherence Tomography-Guided Stentless Strategy
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00020. Epub January 27, 2026.
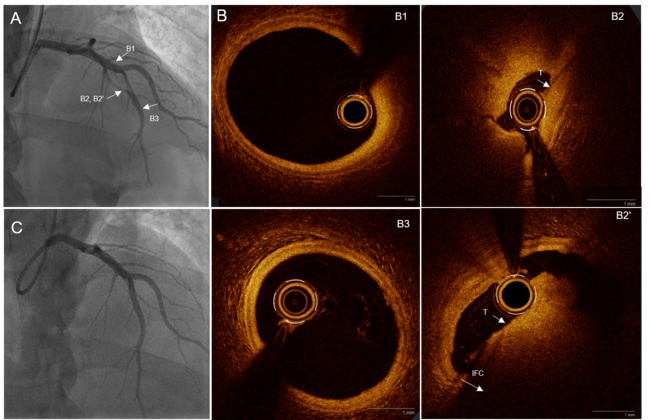
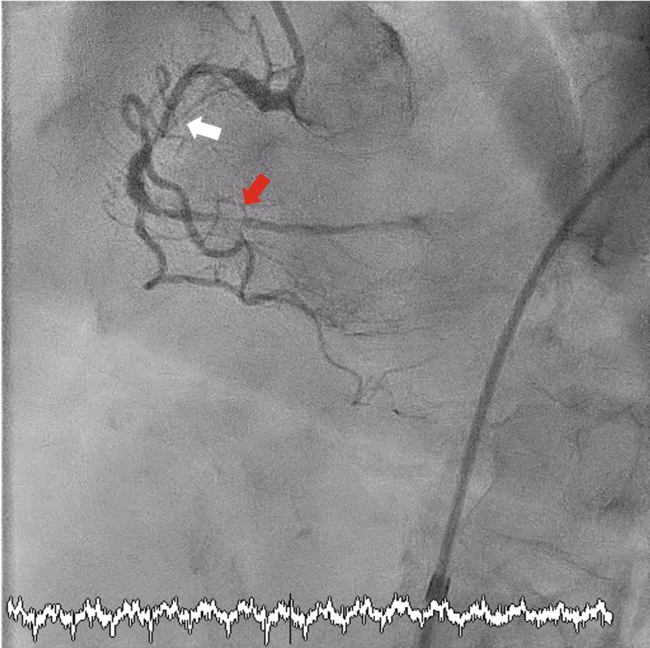
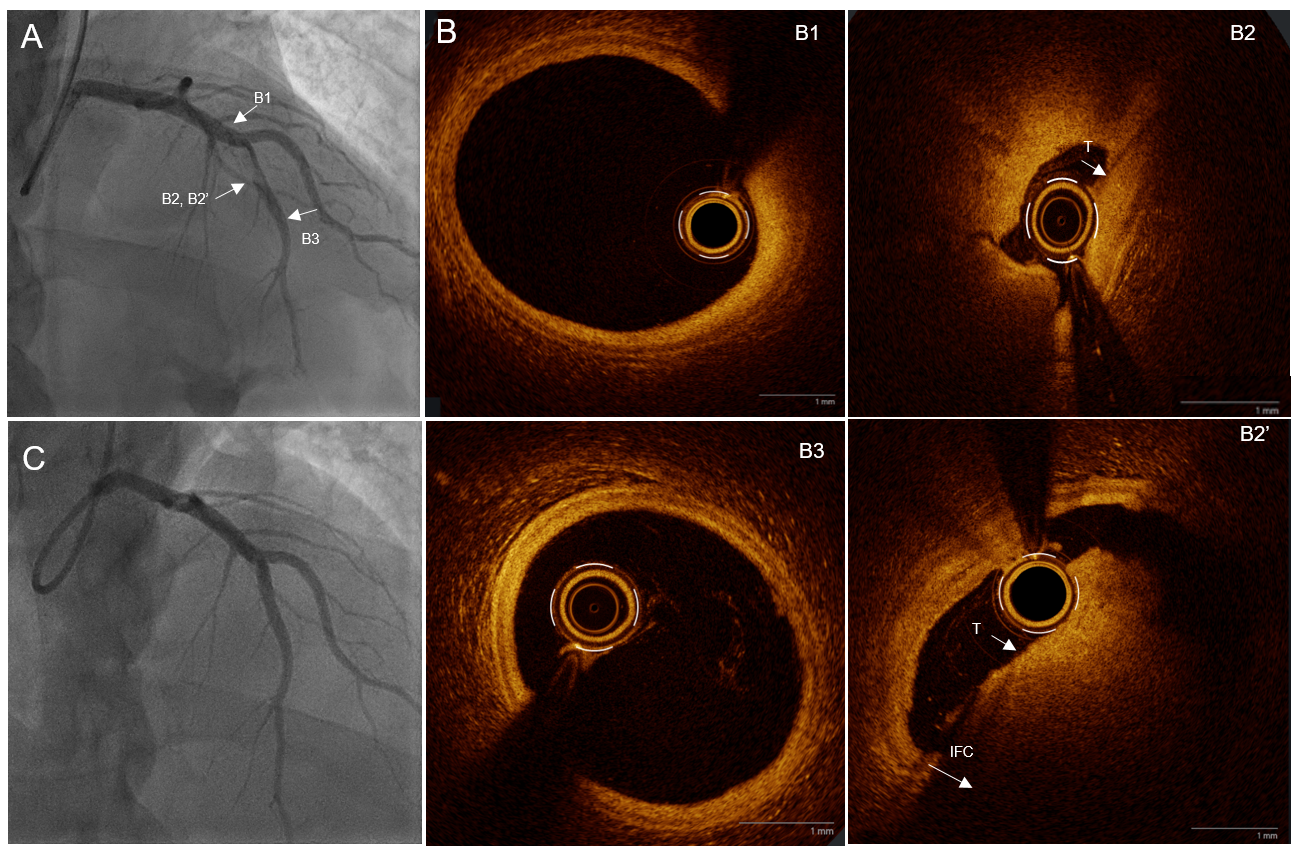
A 28-year-old man with no cardiovascular risk factors presented with an acute anterior ST-elevation myocardial infarction at H+6 after strenuous physical exertion (lifting an extremely heavy load). Emergent angiography revealed a 99% subocclusive stenosis of the mid-left anterior descending (LAD) artery involving a major bifurcation. While distal LAD Thrombolysis in Myocardial Infarction flow was severely impaired, flow in the large diagonal branch remained preserved (Figure A, Video 1).
Optical coherence tomography (OCT) was performed to identify the underlying mechanism. The procedure (crossing the lesion and contrast injections) was associated with mechanical reperfusion. The morphological assessment confirmed an intact fibrous cap diagnostic of plaque erosion. Comparison with the initial luminal narrowing (minimal lumen area [MLA] 0.9 mm²) demonstrated a significant mechanical luminal gain, with a post-reperfusion MLA of 2.6 mm² (Video 2). Precise measurements using the external elastic membrane identified a proximal LAD diameter of 4.4 mm and a distal diameter of 3.4 mm (Figure B).
Given the complexity of the bifurcation and the favorable anatomical result after mechanical reperfusion, a stentless strategy was adopted. Management was exclusively pharmacological, maintained with dual antiplatelet therapy (aspirin 75 mg QD and ticagrelor 90 mg BID) and full anticoagulation with enoxaparin for 8 days. Notably, no glycoprotein IIb/IIIa inhibitors were used. Extensive thrombophilia workup was negative. Follow-up angiography at day 8 showed complete resolution of the thrombus and a strictly normal angiographic appearance (Figure C, Video 3).
At the 30-month follow-up, the patient remained asymptomatic and had fully resumed his heavy professional duties as a forester. A maximal stress test was strictly negative for ischemia, and rest echocardiography confirmed a stable left ventricular ejection fraction of 60%.
Affiliations and Disclosures
Kaïs Ouerghi, MD; Tahar Lazizi, MD; Victor Mateus, MD
From the Department of Interventional Cardiology, Centre Hospitalier de Laval, Laval, France.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the interventions described in the manuscript and for the publication of the patient’s data, including all images and videos.
Address for correspondence: Kaïs Ouerghi, MD, Department of Interventional Cardiology, Centre Hospitalier de Laval, 33 Rue du Haut Rocher, 53000 Laval, France. Email: ouerghi_kais@hotmail.fr