

Intravascular Ultrasound-Guided Management of Early Stent Thrombosis Secondary to Coronary Intramural Hematoma
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00019. Epub January 26, 2026.
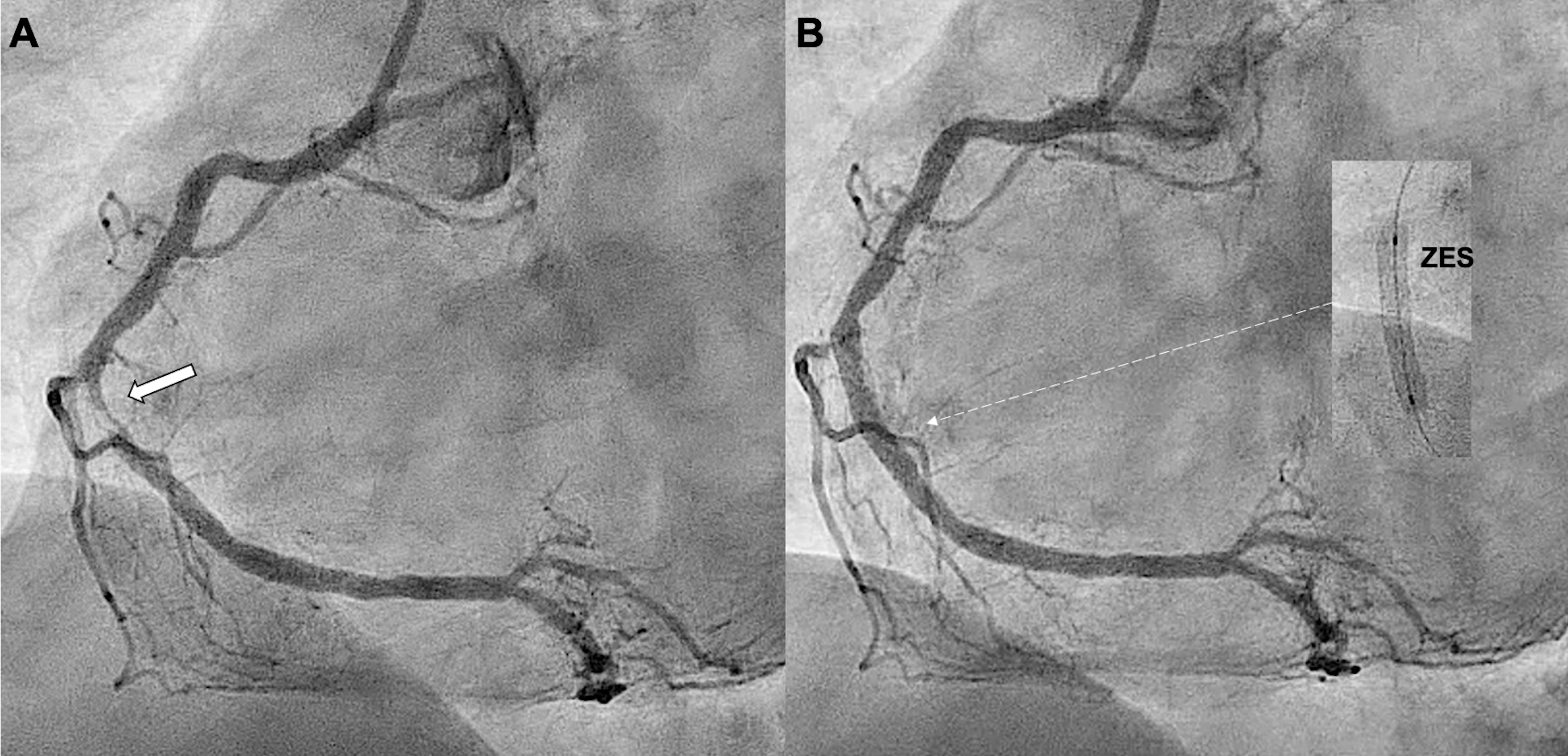
A 42-year-old man was admitted with an inferior ST-segment elevation myocardial infarction. Emergency coronary angiography (CAG) revealed a critical lesion of the middle right coronary artery (RCA) (Figure 1A), which was treated with a 3.5 x 18-mm zotarolimus-eluting stent (ZES) (Figure 1B, Video 1).
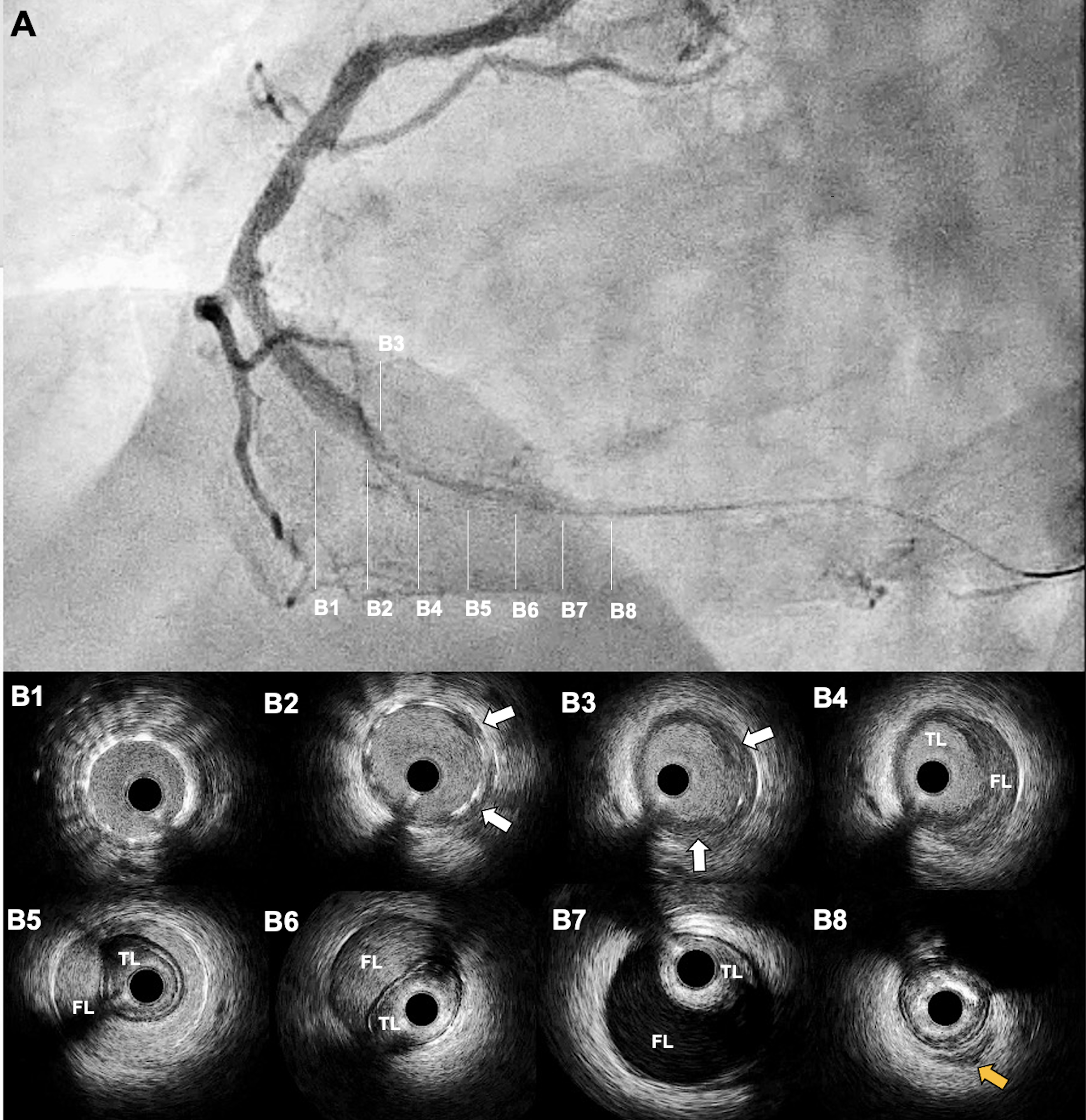
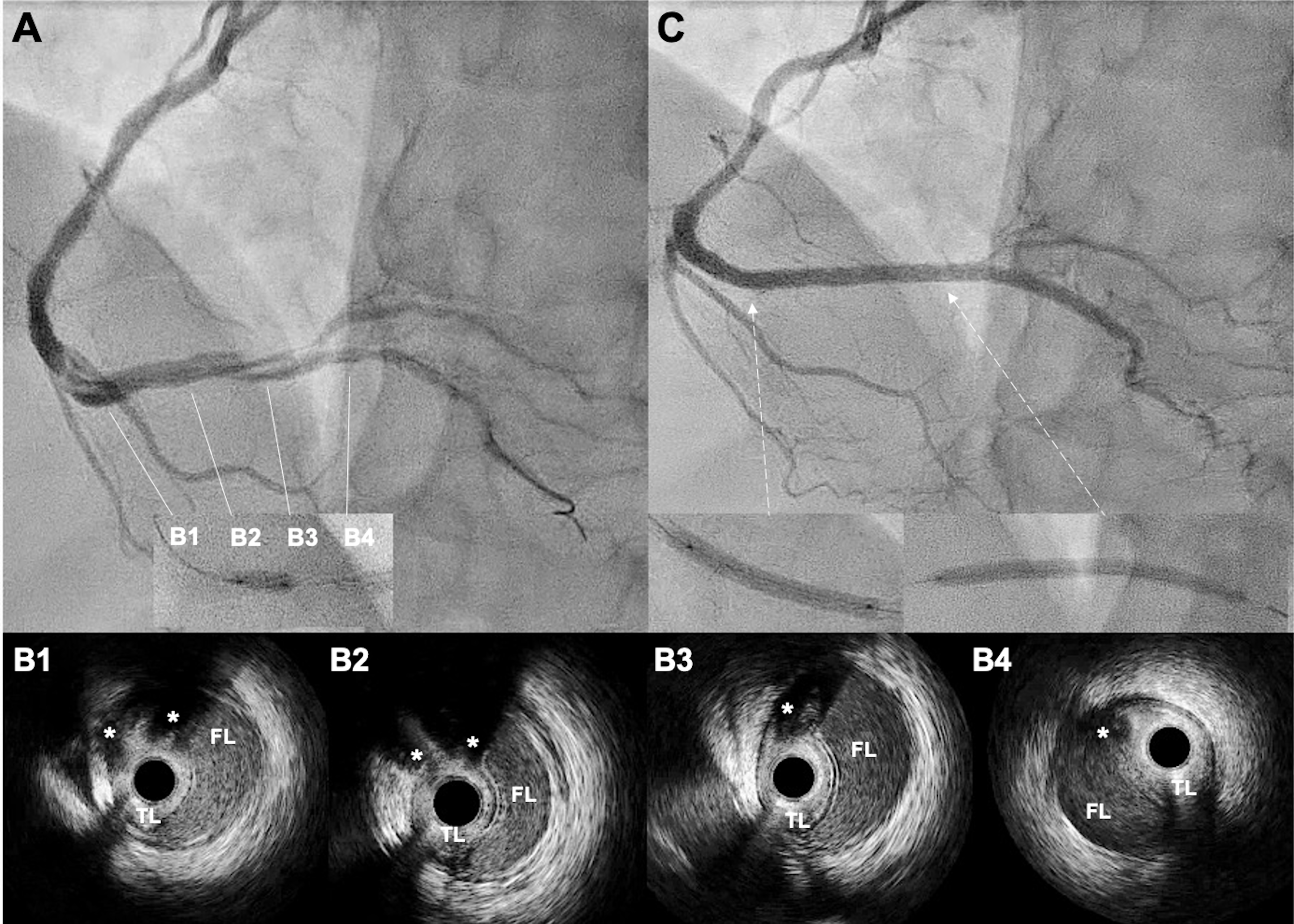
Two hours later, the patient developed recurrent chest pain with inferior ST-segment re-elevation. Repeat CAG revealed acute stent thrombosis (AST) (Figure 2A, Video 2). Thrombus aspiration was performed, and intravascular ultrasound (IVUS) showed a large diffuse intramural hematoma (IH) distal to the ZES, without underexpansion or malapposition (Figure 2B). The IH was fenestrated using a 3.5 x 6.0-mm cutting balloon (Figure 3A, Video 3). Repeat IVUS confirmed multiple fenestration tracts (Figure 3B, Video 4). Two additional overlapping ZES were successfully implanted (Figure 3C). The patient was discharged uneventfully after 48 hours and remained asymptomatic at the 1-month follow-up.
IH is a rare cause of AST that results from subintimal blood propagation beyond the stent edge, leading to luminal compression. Angiography often underestimates IH, which makes IVUS essential for diagnosis and procedural guidance. This case highlights the importance of intracoronary imaging, supports balloon fenestration for IH, and emphasizes it as a treatable but underrecognized complication.
Affiliations and Disclosures
Mireia Martínez, MD1; Paula Vela, MD1; Juan Casanova-Sandoval, MD, PhD1,2; Kristian Rivera, MD1,2
From the 1Department of Cardiology, Arnau de Vilanova University Hospital, Lleida, Spain; 2Grup de Fisiologia i Patologia Cardíaca, Institut de Recerca Biomèdica de Lleida Fundació Dr. Pifarré, IRBLleida, Lleida, Spain.
Disclosures: The authors report that they have no financial relationships or conflicts of interest with respect to the content herein.
Ethics statement: This article was carried out in accordance with the local ethics committee regulations and the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans.
Consent statement: The patient provided his signed informed consent for publication.
Address for correspondence: Kristian Rivera, MD, Arnau de Vilanova University Hospital, Av. Alcalde Rovira Roure, 80, Lleida 25198, Spain. Email: psrivera.lleida.ics@gencat.cat; X: @NoReflow












