Finding the Optimal Pacing Threshold and Avoiding Multiple Deployments of the Micra Device Using Temporary Venous Pacing Mapping
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2025. doi:10.25270/jic/25.00381. Epub December 29, 2025.
A 65-year-old man with complete heart block presented with syncope. He refused a transvenous pacemaker and accepted only a leadless device. At the time, the Micra AV (Medtronic) was the only leadless pacemaker available in the hospital.
The initial Micra AV was implanted with a pacing threshold of 1.0V at 0.4 milliseconds. During follow-up, the threshold fluctuated between 1.5V and 2.0V at 0.4 milliseconds without evidence of gross dislodgement. High pacing dependency and elevated threshold resulted in early battery depletion within 5 years.
A new Micra AV implantation was planned. Given the patient’s relatively young age, the goal was to achieve the lowest possible pacing threshold while avoiding multiple deployments that could dislodge the existing device.
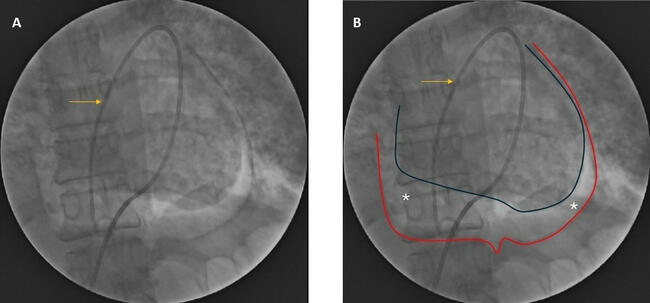
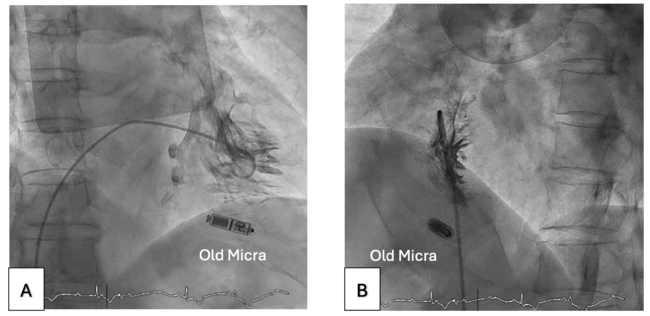
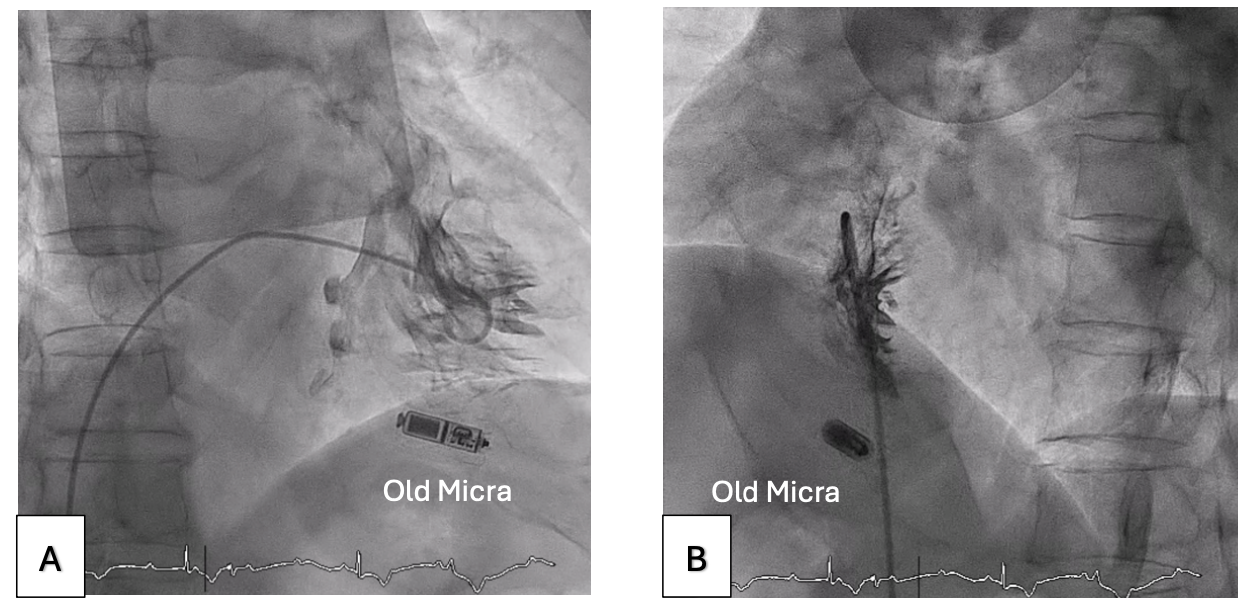
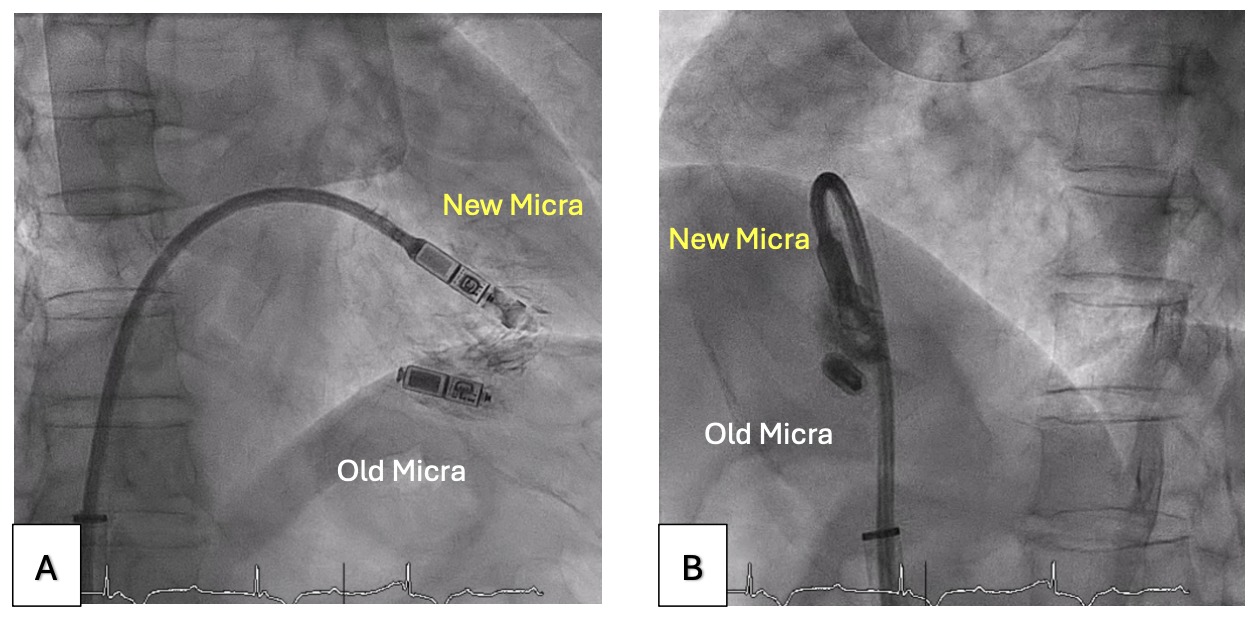
Right ventriculography was performed via right femoral venous access to outline the right ventricular (RV) septum (Figure 1, Video 1). A 5F Arrow temporary venous pacing (TVP) catheter (Teleflex) was then used to measure the pacing thresholds at multiple sites along the RV septum. The site with the lowest threshold was identified and fluoroscopically roadmapped in right and left anterior oblique (LAO) views to guide deployment (Figure 2, Video 2). The venous sheath was exchanged for the 23F Micra delivery sheath, and the new Micra AV was successfully deployed at the pre-identified site (Figure 3, Video 3), achieving a pacing threshold of 0.5V at 0.24 milliseconds and an estimated battery longevity of greater than 10 years.
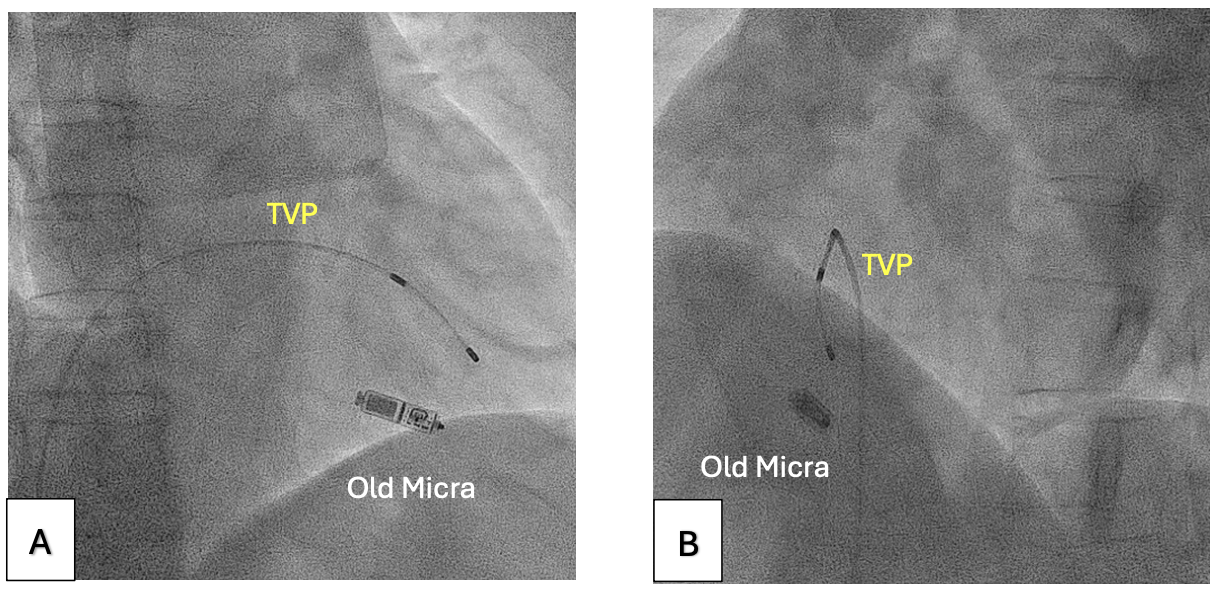
TVP enables rapid testing of pacing thresholds at various sites, allowing identification of the site with the lowest threshold before Micra AV deployment. Although no contrast is used to mark the TVP tip position, its relationship to surrounding anatomical landmarks (eg, ribs, vertebrae) can be noted under consistent fluoroscopic angles and table height. Maintaining these imaging parameters during Micra AV deployment ensures accurate targeting of the optimal site. This method is also applicable when the pacing threshold remains suboptimal after multiple Micra AV deployment attempts. In such cases, a large-bore sheath (eg, 16F) can be inserted into the 23F Micra AV delivery sheath to prevent back-bleeding. A 5F or 6F sheath is then inserted into the 16F sheath, enabling insertion of the TVP catheter to map and identify an optimal pacing site.
The TVP catheter mapping technique can identify the implantation site with the optimal pacing threshold for the Micra AV device and reduce the need for multiple deployments.
Affiliations and Disclosures
Kwok-Ho Yau, MBBS; Tin-Yau Chan, MBBS; Kwok-Keung Chan, MBBS
From the Cardiology Team, Department of Medicine, Pamela Youde Nethersole Eastern Hospital, Chai Wan, Hong Kong SAR.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient(s) for the study and/or intervention(s) described in the manuscript and for the publication of their data/thereof, including any and all images.
Adress for correspondence: Kwok-Ho Yau, MBBS, 3 Lok Man Road, Chai Wan, Hong Kong. Email: jason200200200@hotmail.com