Very Late Thrombosis of a Hemi-Cabrol Coronary Graft: A Rare Cause of Cardiogenic Shock
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/25.00390. Epub January 9, 2026.
A 58-year-old man with a history of ascending aortic aneurysm repair in 2008, including a 26-mm Dacron graft and right coronary artery reimplantation, underwent redo surgery in 2023 because of severe aortic regurgitation. A mechanical valved conduit and a hemi-Cabrol graft from the left main coronary artery (LMCA) to the prosthetic aortic root were implanted. The patient was on chronic, well-adhered coumarin therapy.
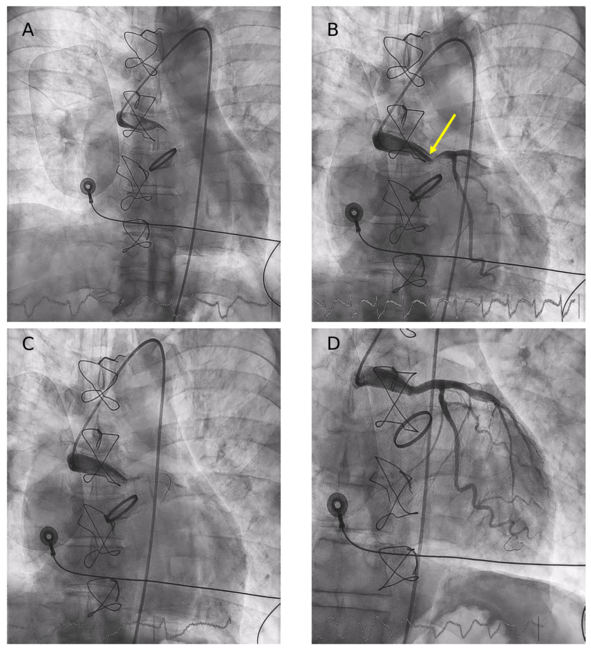
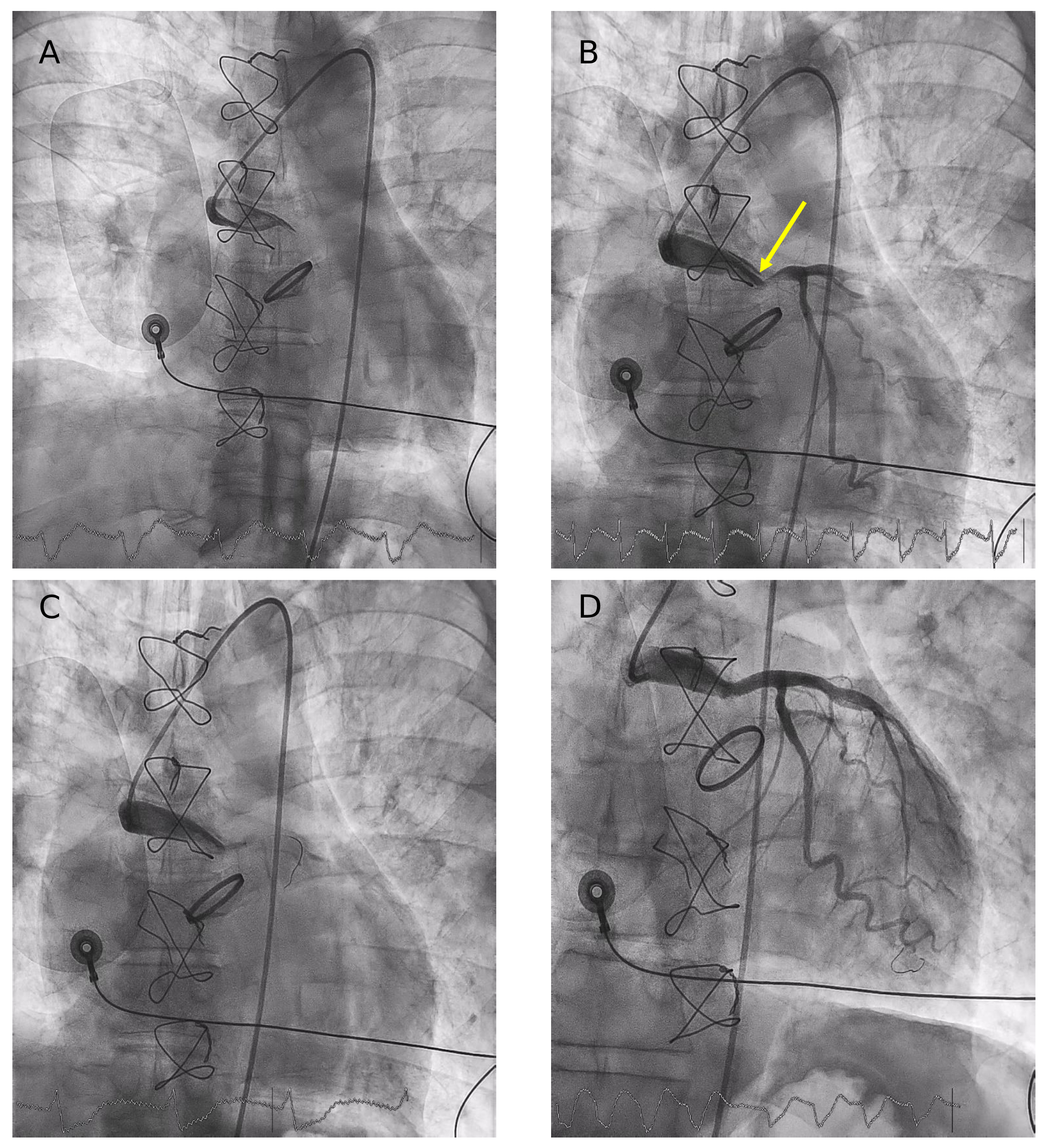
Two years later, he presented to the emergency department with an anterior ST-segment elevation myocardial infarction complicated by cardiogenic shock SCAI (Society for Cardiovascular Angiography & Interventions) stage C. Emergent coronary angiography revealed a subtotal occlusion of the hemi-Cabrol graft caused by a large thrombus, resulting in complete LMCA occlusion. After a challenging catheterization with a 6F JL4 catheter, predilatation was performed using a 2-mm balloon, and 2 overlapping zotarolimus-eluting stents were implanted, followed by partial thromboaspiration because of a residual thrombus (Figure 1, Videos 1-3).
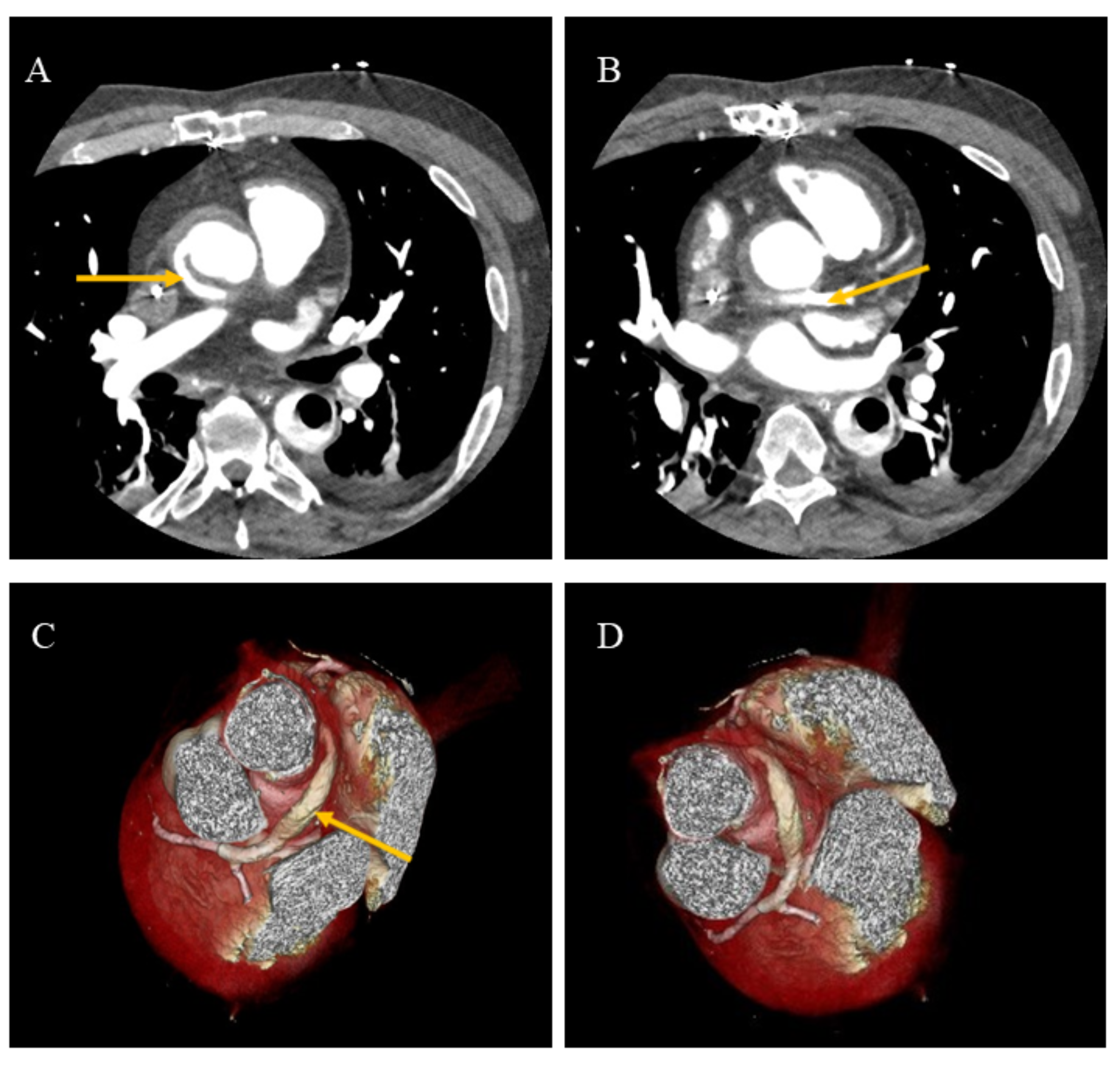
Because of pulseless ventricular arrhythmias, the patient required intubation and support with femoro-femoral veno-arterial extracorporeal membrane oxygenation (VA-ECMO) combined with an intra-aortic balloon pump. Cardiac computed tomography performed several days later confirmed the patency of both stents and the anatomical configuration of the graft (Figure 2).
Three weeks later, the patient underwent urgent heart transplantation because of extensive myocardial damage and the inability to wean from VA-ECMO; however, he ultimately died from severe postoperative complications.
Cabrol graft thrombosis more commonly affects the right coronary artery1 and thrombosis of the LMCA is very rare.2 To our knowledge, this is the first reported case of LMCA thrombosis in the context of a hemi-Cabrol graft and mechanical aortic valve requiring both thromboaspiration and VA-ECMO support.
Affiliations and Disclosures
Miguel A. Martín-Arena, MD1; Joaquín Vila-García, MD1; Clara Ugueto-Rodrigo, MD1,2; Cristina Contreras-Lorenzo, MD1,2; Ricardo Martínez-González, MD1; Carmen Labarta-Bello, MD1; Guadalupe Buitrago Weiland, MD3; Sandra Rosillo-Rodríguez, MD, PhD1,2; Santiago Jiménez-Valero, MD1,2; Raúl Moreno, MD, PhD1,2
From the 1Department of Cardiology, La Paz University Hospital, Madrid, Spain; 2Research Institute of La Paz University Hospital (IdiPAZ), Madrid, Spain; 3Department of Radiology, La Paz University Hospital, Madrid, Spain.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript. Following the patient’s death, consent for the use of images and publication of the case was obtained from the family.
Address for correspondence: Miguel A. Martín-Arena, MD, Department of Cardiology, La Paz University Hospital, Paseo de la Castellana 261, Madrid 28046, Spain. Email: miguelangelmartinarena@gmail.com; X: @martinarenaMA
References
- Poullis M, Pullan M. Mechanism of failure of the Cabrol procedure: a computational fluid dynamic analysis. Med Hypotheses. 2015;85(6):774-778. doi:10.1016/j.mehy.2015.10.010
- Hsiao YW, Huang JW. Myocardial ischemia 10 years after a modified Cabrol procedure in a 42-year-old patient with Marfan syndrome. BMC Cardiovasc Disord. 2020;20(1):461. doi:10.1186/s12872-020-01740-6