

Real-Time Intravascular Ultrasound-Assisted Wiring of Subtotal Left Anterior Descending Artery Ostial Lesion to Achieve Percutaneous Coronary Intervention With Minimal Contrast
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
A 51-year-old man presented with non-ST-segment elevation myocardial infarction (NSTEMI). He had a medical history of diabetes mellitus and severe renal impairment (estimated glomerular filtration rate of 25 mL/min/1.73 m²).
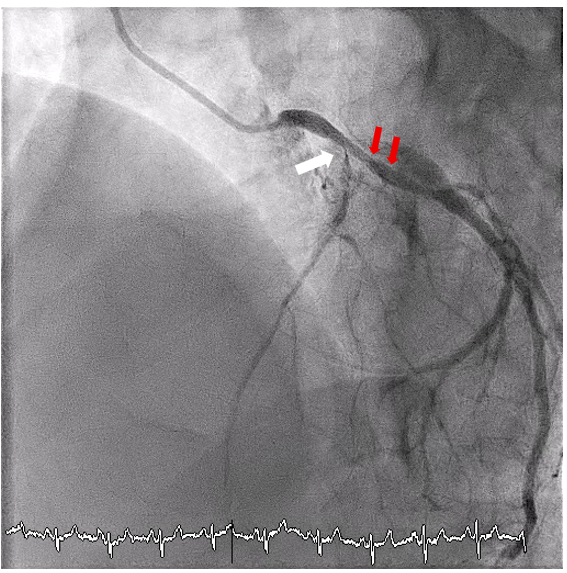
Coronary angiography revealed subtotal occlusion at the ostium of the left anterior descending artery (LAD) (Figure 1). Percutaneous coronary intervention (PCI) was initiated, aiming at minimal contrast use. Using a 7F Extra Back-Up guiding catheter (Medtronic), the left circumflex artery (LCx) was first wired for protection. A SASUKE dual-lumen microcatheter (ASAHI INTECC) was inserted into the LCx, and an attempt was made to wire the LAD using a polymer-jacketed FIELDER FC wire (ASAHI INTECC) through the dual-lumen microcatheter. However, wiring the ostial LAD lesion proved challenging without contrast injection. There was no obvious landmark (eg, calcium) at the ostial LAD, and the wire easily got into 2 small branches that were present near the ostium (Figure 1), the course of which was easily mistaken as the LAD. It was essential to confirm that the wire was in the LAD before stepping up to a penetrating wire.
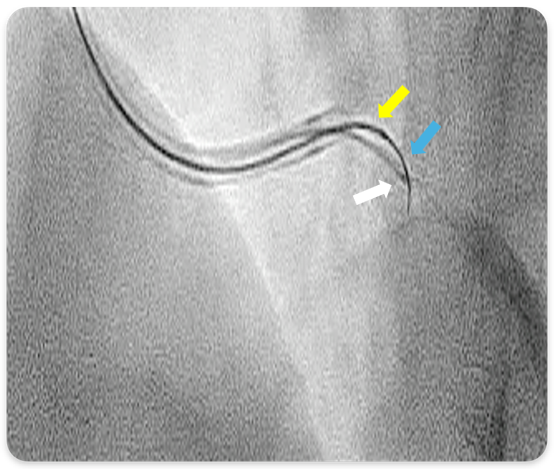
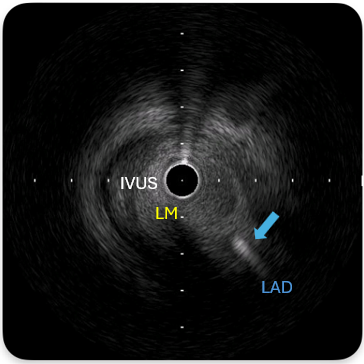
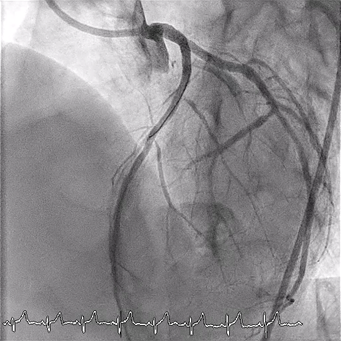
Real-time intravascular ultrasound (IVUS)-guided wiring of the LAD was then planned. An AltaView IVUS catheter (Terumo) was placed at the LCx wire. The IVUS lens served as a landmark for the ostial LAD. A Gaia Next 1 wire (ASAHI INTECC) supported by a single-lumen Hightrack microcatheter (Terumo) was then used to wire the ostial LAD (Figure 2). The Gaia Next 1 wire successfully crossed the ostial LAD lesion, as confirmed by IVUS (Figure 3). It was subsequently exchanged for a Gaia Next 2 (ASAHI INTECC) wire through the microcatheter to address another tight lesion in the proximal LAD. The procedure was completed successfully following balloon dilatation and stenting (Figure 4). The total amount of contrast use was 35 mL.
This case illustrates how real-time IVUS can assist in wiring as a contrast-saving strategy. A 7F guiding catheter is required for the concomitant use of the AltaView IVUS and a single-lumen microcatheter. Recommended microcatheters include the Hightrack, FineCross MG (Terumo), and Caravel (ASAHI INTECC).
Affiliations and Disclosures
Kwok-Ho Yau, MBBS; Justin Ka-Ho Wong, MBBS; Tin-Yau Chan, MBBS; Kin-Lam Tsui, MBBS, FACC
From the Cardiology Team, Department of Medicine, Pamela Youde Nethersole Eastern Hospital, Chai Wan, Hong Kong SAR.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient(s) for the study and/or intervention(s) described in the manuscript and for the publication of their data/thereof, including any and all images.
Address for correspondence: Kwok-Ho Yau, MBBS, 3 Lok Man Road, Chai Wan, Hong Kong. Email: jason200200200@hotmail.com













