Not All Kisses are the Same: Kissing Balloon Inflation in the Left Main Coronary Artery With Ultra High-Pressure Noncompliant Balloons
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00033. Epub February 13, 2026.
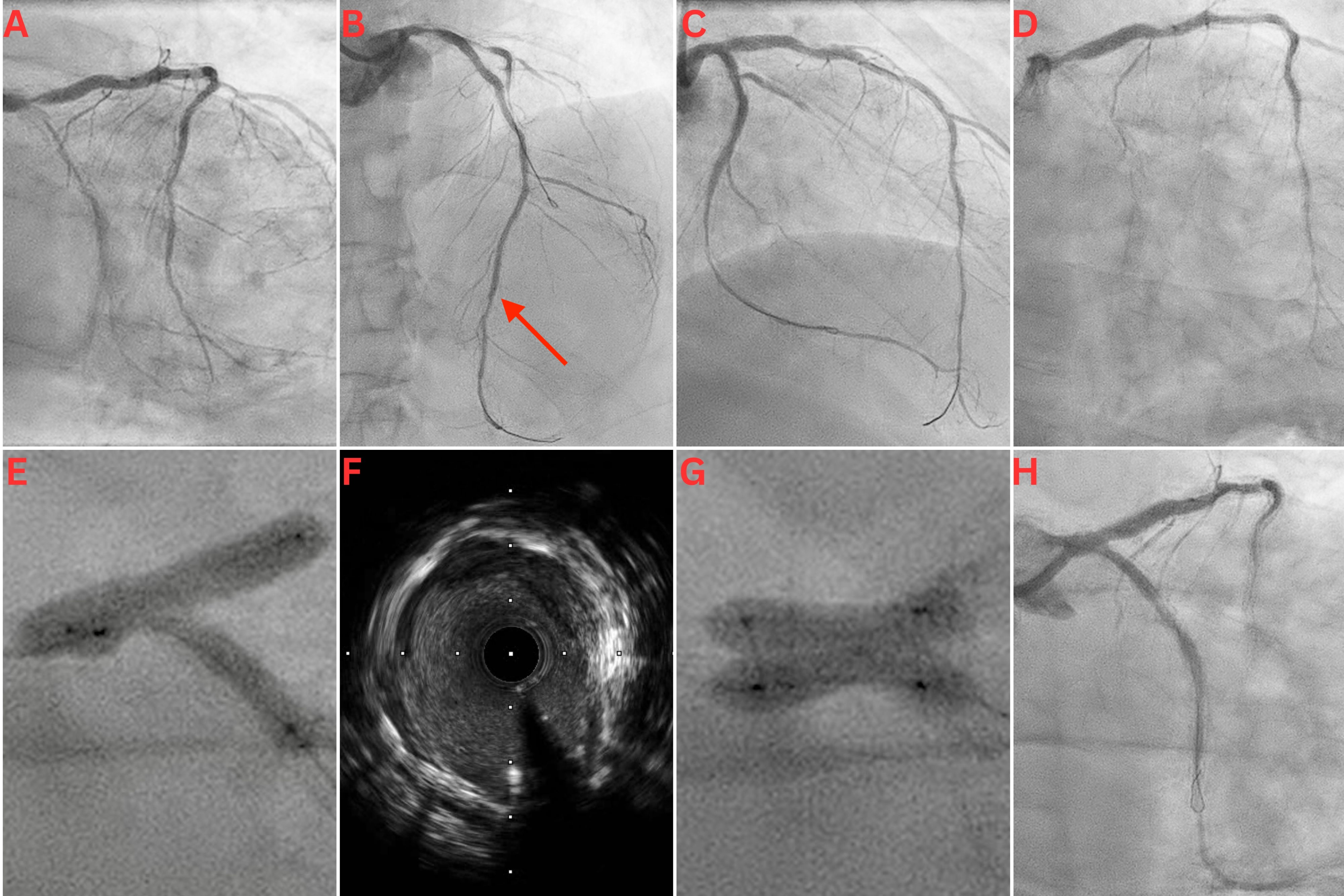
A 65-year-old man with a history of extensive percutaneous coronary intervention (PCI) because of recurrent in-stent restenosis (ISR) presented with a non-ST segment elevation myocardial infarction (NSTEMI). Coronary angiography revealed severe ISR in his left main coronary (LMCA), left anterior descending (LAD), and left circumflex (LCx) arteries (Figure A and B). Intravascular ultrasound (IVUS) revealed an LMCA diameter of 5.5 mm, deep vessel calcification, and severe neo-intimal hyperplasia, with only mild stent underexpansion. IVUS-guided PCI of the LMCA, LAD, and LCx was performed using a scoring balloon, a 5.5-mm noncompliant (NC) balloon in the LMCA, and 4.0 and 3.5-mm Paclitaxel drug-eluting balloons (DEB) in the LAD and LCx, respectively. There was a good final angiographic result following this intervention (Figure C).
The patient represented 5 months later with an NSTEMI. Angiogram revealed critical ISR of the recently treated LMCA bifurcation (Figure D). PCI was performed using NC and cutting balloons, followed by several applications of excimer laser coronary atherectomy (ELCA) in the LMCA, LAD, and LCx. Three-stage kissing balloon inflations (KBI) at the LMCA bifurcation were performed with a 4.0-mm NC balloon in the LAD and a 3.5-mm NC balloon in the LCx. There was significant waisting without complete balloon expansion (Figure E). IVUS showed calcification, stent recoil, and residual neo-intimal hyperplasia (Figure F, Video 1). Following prolonged inflations with 4.0 x 20-mm and 3.5 x 20-mm Paclitaxel DEBs in the LAD and LCx, respectively, two 4.0 x 10-mm OPN NC ultra high-pressure balloons (SIS Medical AG) were used individually for postdilation in both the proximal LCx and LAD; they were each inflated to 40 atm. Finally, KBI was performed in the LMCA/LAD/LCx bifurcation with the 2 OPN balloons to 20 atm each. There was complete balloon expansion with noticeable angiographic improvement (Figure G).
Following ELCA and balloon angioplasty, there was minimal tissue within the stents in either vessel. However, there was significant tissue behind the stent in the LCx, giving the appearance of moderate disease in the mid-LCx on the final angiographic images. Given there was a good minimal luminal area on IVUS, and the patient had a poor response to stents in the past with recurrent ISR, this was accepted as a good final angiographic result at the end of the procedure (Figure H, Video 2). The patient was discharged on dual antiplatelet therapy and colchicine for its antiproliferative effects. He remained well and asymptomatic on review after 6 months.
To the best of our knowledge, this is the first described case of KBI in the LMCA using 2 OPN ultra high-pressure NC balloons. We specifically chose this treatment option because of the extremely high calcium burden increasing the risk of stent recoil and further ISR. Study data reflects a good efficacy and safety profile of OPN balloons, with 95.1% procedural success, 1.9% periprocedural major adverse cardiovascular events, and 0.6% incidence of coronary perforation, with even lower complication rates when intravascular imaging is employed for vessel sizing.1
Affiliations and Disclosures
Gregory Offiah, MB, BCh, BAO, MRCPI; John P. Birrane, BA, BM BS, MCh, MRCPI; Ian Pearson, MB, BCh, BAO, MRCP, MD; John Cosgrave, MB, BCh, BAO, MRCPI, MD
From the Cardiology Department, St James’s Hospital, Dublin 8, Ireland.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: Informed consent was obtained from the patient for the publication of this case
Address for correspondence: Gregory Offiah, MB, BCh, BAO, MRCPI, Department of Cardiology, St James’s Hospital, Dublin 8, D08 NHY1, Ireland. Email: goffiah@tcd.ie; X: @gregoffiah
References
1. Kumar S, Jalli S, Sandoval Y, et al. Systematic review and meta-analysis of the super high-pressure balloon (SIS-OPN) for percutaneous coronary intervention. Catheter Cardiovasc Interv. 2025;105(4):938-950. doi:10.1002/ccd.31403