Subaortic Membrane Recurrence With Obstructive Physiology
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/25.00399. Epub February 26, 2026.
A subaortic membrane is a fibrous tissue that forms in the left ventricular outflow tract (LVOT), resulting in subaortic stenosis.1 Recurrence rates after resection vary from approximately 10% to 27% over long-term follow-up.2,3 We report a young patient with regrowth of subaortic membrane 10 years after initial resection, presenting with syncope.
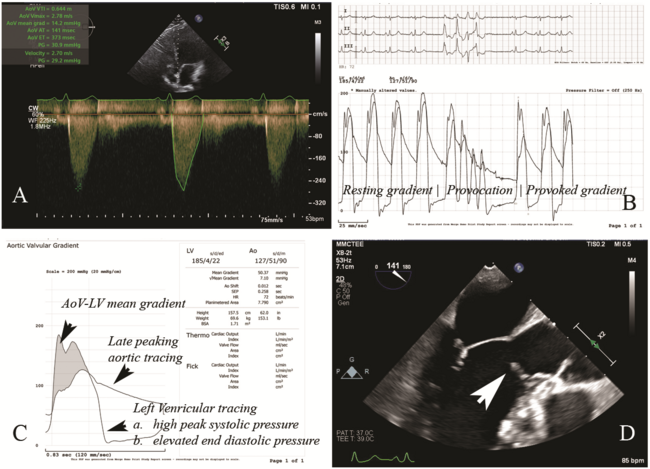
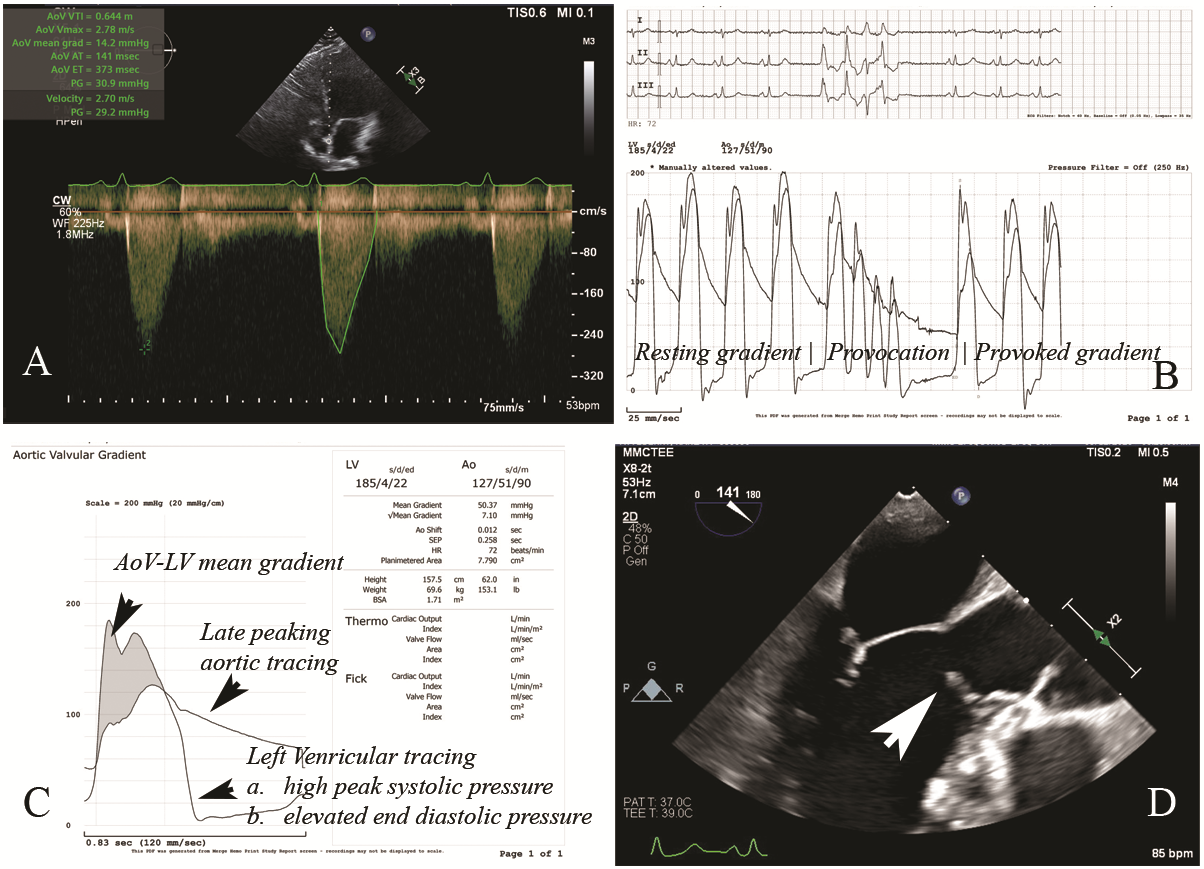
A 42-year-old woman who underwent subaortic membrane surgical resection in 2014 presented with severe dyspnea and recent syncope. Evaluation in the emergency room revealed stable vital signs and unremarkable electrocardiogram and cardiac biomarkers. Transthoracic echocardiogram showed an aortic valve (AoV) peak velocity of 2.78 m/s, a peak gradient (PG) of 31 mm Hg, a mean gradient of 14 mm Hg, and an AoV area of 2.09 cm² (Figure A). There were elevated pressure gradients across the LVOT and AoV, with a PG of 31 mm Hg at rest.
Regrowth of subaortic membrane was suspected given the normal AoV morphology and elevated gradients. Cardiac catheterization demonstrated normal coronary arteries, but an elevated left ventricular end-diastolic pressure at 30 mm Hg. Resting and provoked LVOT gradient were elevated at 20 and 50 mm Hg, respectively (Figure B and C). Transesophageal echocardiogram (TEE) revealed regrowth of subaortic membrane in the LVOT (Figure D). Video 1 shows the mid-esophageal long-axis view through the LVOT and aortic valve. Additionally, Video 2 shows the mid-esophageal long-axis view through the LVOT and aortic valve; X-plane focused at the subaortic membrane and color flow Doppler is shown in Video 3.
The patient successfully underwent a redo resection by cardiothoracic surgery. Intraoperative TEE revealed a subaortic membrane extending from the proximal part of LVOT to the mitral annulus with a gradient of 20 mm Hg across the membrane. Intraoperative findings after aortotomy with the right coronary cusp retracted anteriorly showed a mid-ventricular subaortic membrane, which was excised sharply in its entirety. The portion of membrane at the anterior leaflet of the mitral valve was excised, after which the LVOT was widely patent. Post-resection TEE confirmed removal of the membrane with a residual gradient of 10 mm Hg, likely due to a hyperdynamic left ventricular ejection fraction. At her 1-month surgical follow-up, the patient reported significant improvement in dyspnea.
Affiliations and Disclosures
Soomal Rafique, MD1; Rami Al-Ayyubi, MD2; Dylan Thompson, MD3; William Stevens, MD4; Abdul Moiz Hafiz, MD2
From the 1Department of Internal Medicine, Southern Illinois University School of Medicine, Springfield Illinois; 2Division of Cardiology, Southern Illinois University School of Medicine, Springfield, Illinois; 3Southern Illinois University, School of Medicine, Springfield, Illinois; 4Cardiothoracic Surgery, Department of Surgery, Southern Illinois University School of Medicine, Springfield, Illinois.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: An informed consent was obtained from the patient.
Data availability statement: The data underlying this article cannot be shared publicly due to privacy of the patient. The data will be shared upon a reasonable request to the corresponding author.
Address for correspondence: Soomal Rafique, MD, Department of Internal Medicine, Southern Illinois University School of Medicine, 751 N. Rutledge, Springfield, Illinois 62702, USA. Email: srafique73@siumed.edu; X: @RafiqueSoomal
References
1. Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;73(12):e81-e192. doi:10.1016/j.jacc.2018.08.1029
2. Talwar S, Anand A, Gupta SK, et al. Resection of subaortic membrane for discrete subaortic stenosis. J Card Surg. 2017;32(7):430-435. doi:10.1111/jocs.13160
3. Mazurek AA, Yu S, Lowery R, Ohye RG. Routine septal myectomy during subaortic stenosis membrane resection: effect on recurrence rates. Pediatr Cardiol. 2018;39(8):1627-1634. doi:10.1007/s00246-018-1941-5