


Sex Disparities in Coronary Angiography Findings of Out-of-Hospital Cardiac Arrest Complicating Acute Coronary Syndromes
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Objectives. Sex-based disparities have been widely reported in the management and outcomes of out-of-hospital cardiac arrest (OHCA), often complicating acute coronary syndromes (ACS). While previous studies have demonstrated that female patients are less likely to undergo invasive coronary angiography (ICA) or percutaneous coronary intervention (PCI), little is known about potential differences in coronary anatomy or PCI strategies in this context. The authors sought to evaluate sex-related differences in ICA findings and PCI management among OHCA survivors with angiographically confirmed ACS.
Methods. The authors conducted a retrospective, single-center study including consecutive OHCA patients admitted to the intensive care unit of a tertiary center between 2007 and 2024 who underwent emergent PCI. Propensity score matching was used to compare females and males based on key baseline characteristics. Coronary lesion characteristics, procedural data, and clinical outcomes were analyzed.
Results. Among 486 patients (mean age 60.6 ± 12.2 years), 105 (21.6%) were female patients. After matching, 210 patients (105 female, 105 male) were included. No significant differences were observed in the extent of coronary artery disease, lesion complexity, or PCI strategies. Female patients had more frequent right coronary artery culprit lesions and less left circumflex involvement. Thrombus aspiration was more common in female patients (33.3% vs 21.0%, P = .04). Adjusted in-hospital and 3-month mortality rates were not significantly different.
Conclusions. In OHCA survivors with ACS undergoing PCI, females and males had similar angiographic profiles and PCI approaches. These findings suggest that coronary and procedural factors do not explain sex-based differences in OHCA outcomes, underlining the need for equitable access to early invasive management.
Introduction
Out-of-hospital cardiac arrest (OHCA) remains a major public health issue. It is frequently caused by acute coronary syndromes (ACS) and is associated with high mortality and neurological disability rates.1 Despite advances in resuscitation and post-arrest care, growing evidence has highlighted persistent sex-based disparities in both clinical outcomes and management strategies.2-6
The role of sex has been examined, and some studies have found lower survival rates as well as poorer neurological and functional recovery after OHCA in females compared with males.5,7-9 However, a large meta-analysis found that female patients had more favorable in-hospital prognosis.10 These differences may stem from variations in clinical presentation, such as lower incidence of shockable rhythms and reduced rates of bystander cardiopulmonary resuscitation (CPR) in female patients, but also from disparities in care delivery.4,11,12 Invasive procedures like intensive care unit (ICU) admission, invasive coronary angiography (ICA), percutaneous coronary intervention (PCI), and the use of mechanical circulatory support (MCS) are less frequently performed in female patients.2,3,13
While it is well established that female patients are less likely to undergo ICA following OHCA, it remains unclear whether these disparities extend to the angiographic characteristics of coronary artery disease (CAD) and PCI strategies among patients with confirmed ACS requiring revascularization. Prior studies often included unselected populations, limiting our understanding of sex-based differences in patients who have an indication for revascularization. Clarifying whether anatomical disease burden, lesion complexity, or procedural approaches differ by sex in this high-risk subgroup is essential, as such differences may help explain the poorer outcomes observed in female patients.
In this study, we aimed to investigate sex-based differences in angiographic findings and PCI management among OHCA survivors with confirmed ACS requiring revascularization.
Methods
Study population
We conducted a retrospective, single-center, observational study at a tertiary center in Cochin Hospital (Paris, France), including all consecutive patients admitted to the ICU for OHCA between January 2007 and December 2024. In accordance with European Resuscitation Council and European Society of Intensive Care Medicine guidelines, patients underwent ICA and subsequent PCI if a culprit acute coronary lesion was identified as the cause of the cardiac arrest.14,15 Patients were eligible for inclusion in this study if they were 18 years or older, had achieved return of spontaneous circulation (ROSC), and underwent emergent PCI.
This study was conducted in accordance with the Declaration of Helsinki. The data were collected from the PROCAT registry, which is part of the Cochin Cardiac Arrest database that has been approved by the Ethics Committee of the French Intensive Care Society (CE-SRLF 12-384) (CE-SRLF 12-384).
Data collection and management of patients
Baseline demographics, medical history, and in-hospital outcomes were obtained from medical records. Laboratory values were recorded as the first available measurements after ICU admission. Left ventricular ejection fraction (LVEF) was assessed by echocardiography within 48 hours of admission. The management was left at the discretion of the clinicians, including targeted hypothermia. When initiated, the target temperature was set at 32 °C to 34 °C for 24 hours, in accordance with standard therapeutic hypothermia protocols.
Detailed coronary angiographic data were systematically collected to evaluate the burden and complexity of CAD in this population. Information was obtained from procedural reports and angiographic images, including the extent of CAD (single-, 2-, or 3-vessel disease), location of culprit lesion (left anterior descending, left main, left circumflex [LCx], or right coronary artery [RCA]), presence of bifurcation lesions, chronic total occlusions (CTO), severe calcification, and initial Thrombolysis in Myocardial Infarction (TIMI) flow grade before PCI (≤ 2). We also recorded the number of angiographically unstable lesions. Data related to PCI procedures were also collected, including the number of stents deployed, the number of treated lesions, the use of thrombus aspiration, and the post-PCI TIMI flow grade (≤ 2), as well as the occurrence of no-reflow phenomena.
In-hospital outcomes included all-cause death, bleeding, major bleeding, and definite or probable stent thrombosis. The incidence of 3-month all-cause death was also collected and was ascertained using the French national electronic registry of death (INSEE registry).
Bleeding events were classified using the Bleeding Academic Research Consortium (BARC) classification, which ranges from type 1 to type 5.16 In our study, types 3, 4, and 5 were considered as major bleeding events. In cases of multiple bleeding events, the most serious event was considered for analysis.
Stent thrombosis was defined according to the ARC for stents trials as 1) definite if the patient had an MI with angiographic or pathologic confirmation of the thrombus; 2) probable in cases of unexplained death within 30 days or MI in the target vessel territory without angiographic confirmation.17
Statistical analysis
Descriptive statistics were performed, with continuous variables expressed as means and standard deviations or medians and interquartile ranges, and categorical variables expressed as counts and percentages. Comparative analyses were conducted using Student’s t-test or Wilcoxon rank-sum test for continuous variables, and chi-squared tests or Fisher’s exact tests for categorical variables as appropriate.
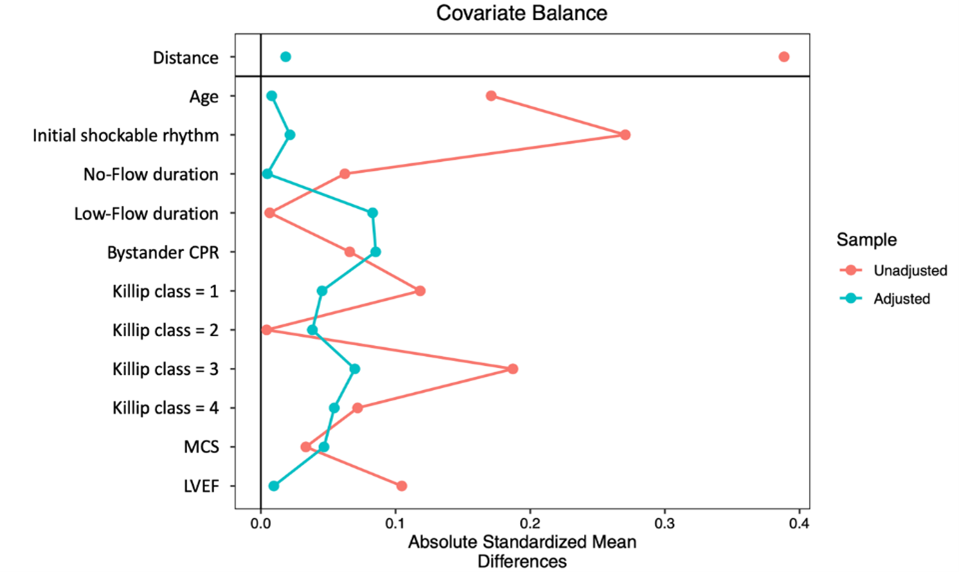
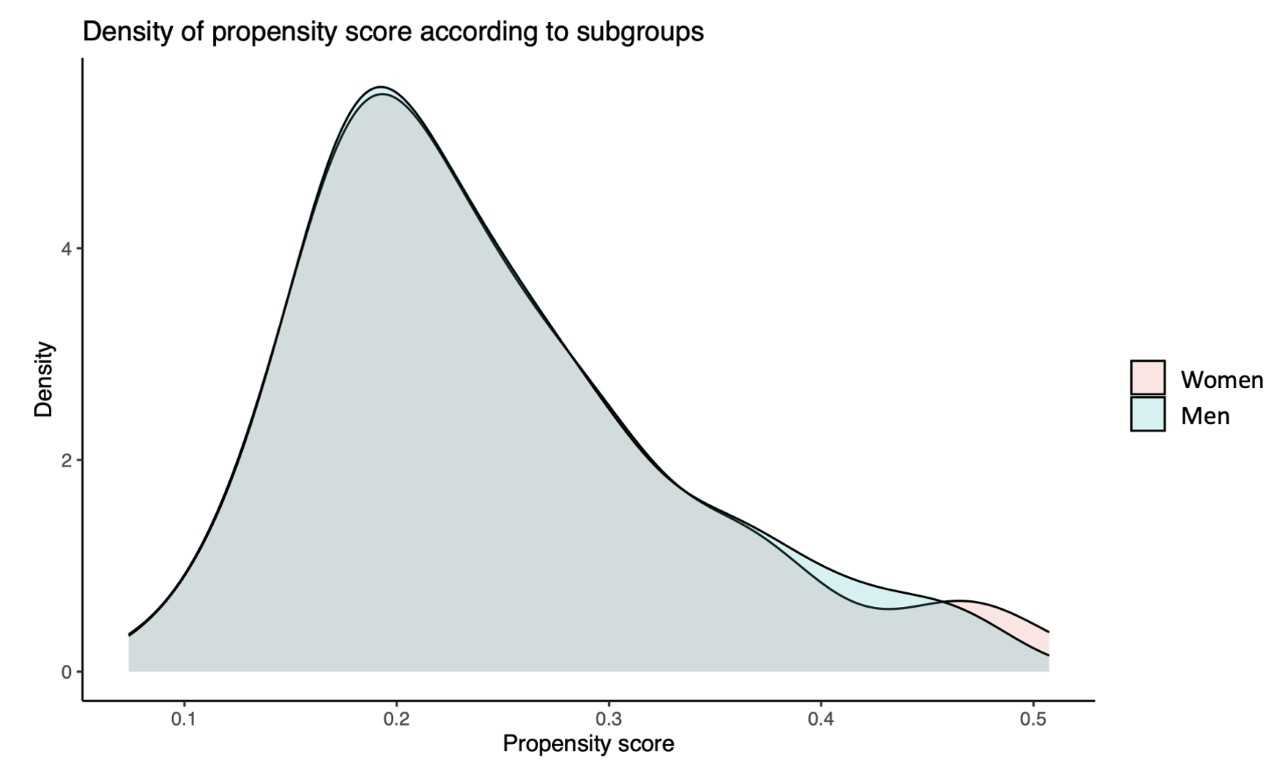
To compare ICA and PCI data between female and male patients, propensity score matching was performed at a 1:1 ratio using logistic regression to adjust for the following baseline characteristics: age, presence of shockable rhythm, time from arrest to CPR and time from CPR to ROSC durations, bystander CPR, Killip class, use of MCS, and LVEF (Supplemental Figure 1).
The association between sex and outcomes was assessed using univariable and multivariable logistic regression or Cox proportional hazards regression models for in-hospital and 3-month outcomes, respectively. Multivariable analyses were adjusted for potential confounders defined a priori and based on existing literature. These included age, shockable initial rhythm, no-flow and low-flow durations, bystander CPR, Killip class, noradrenaline and dobutamine use, MCS, LVEF, pH, lactate, and troponin.
A 2-sided P-value of less than 0.05 was considered significant. All analyses were conducted using R software version 3.6.0 (R Foundation for Statistical Computing).
Results
Study population
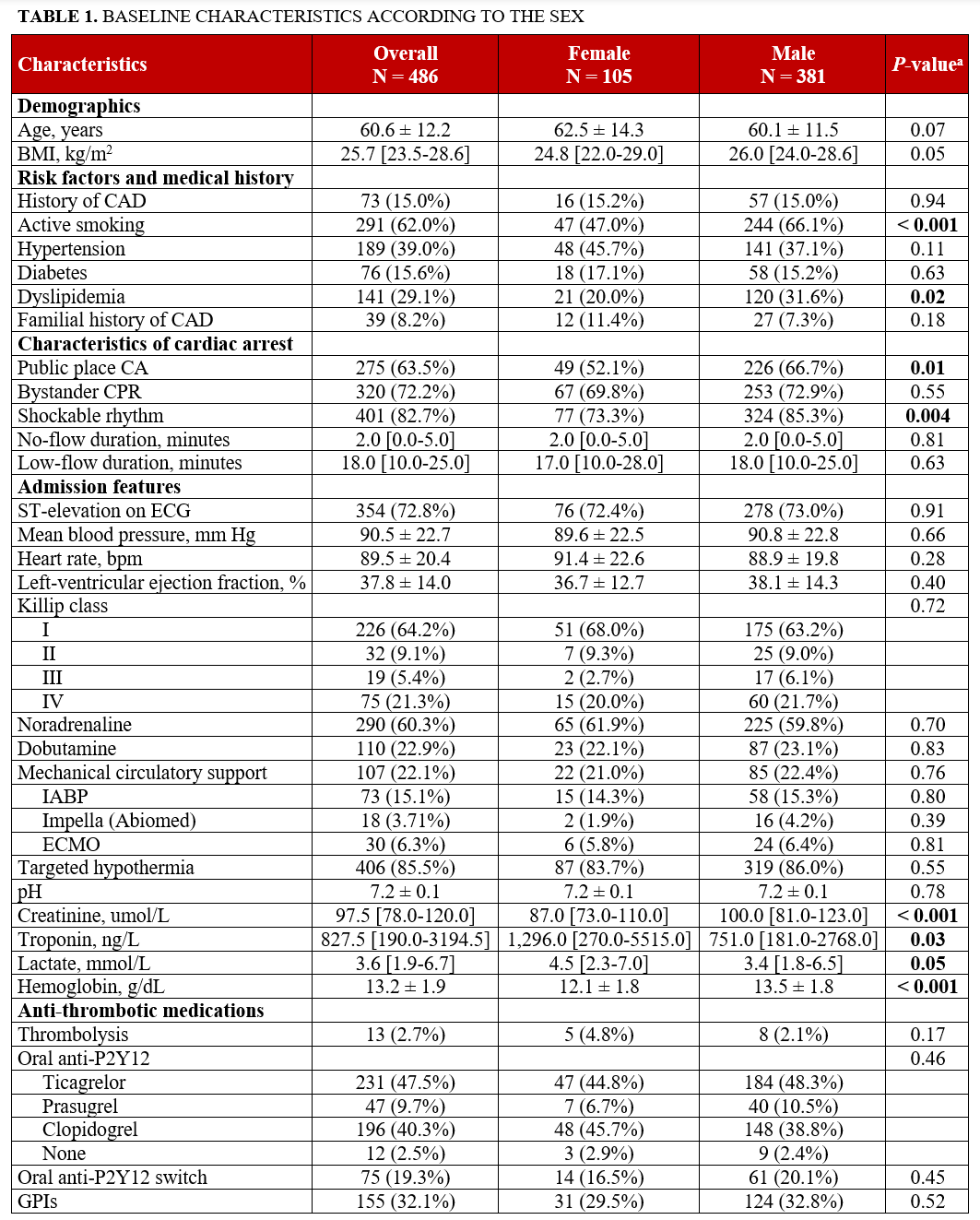
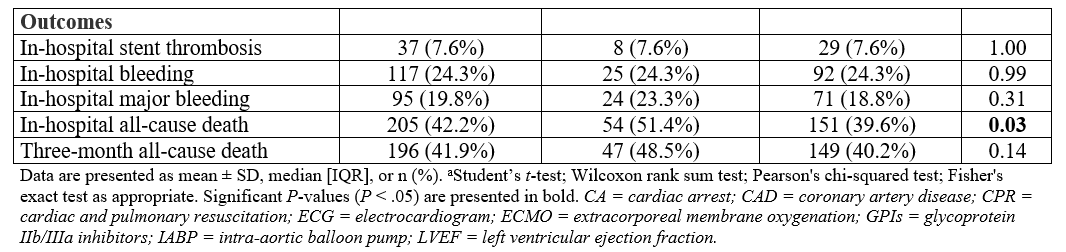
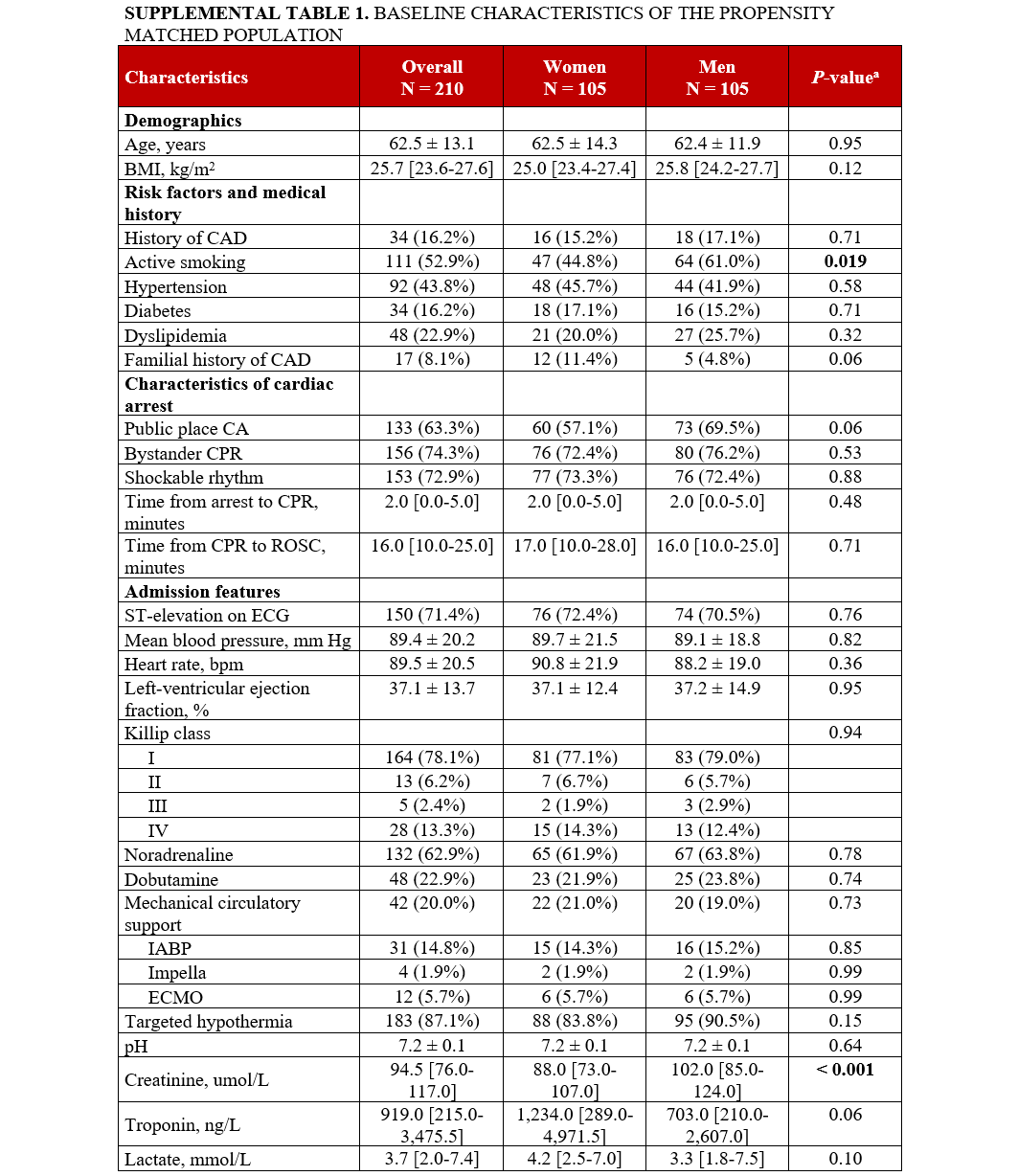
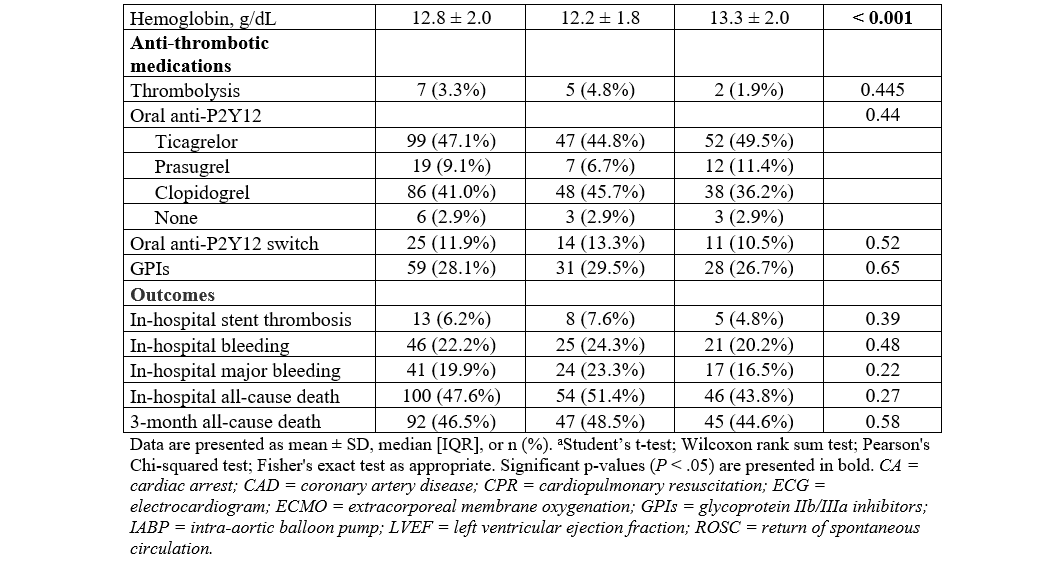
A total of 486 patients with OHCA complicating ACS and who underwent PCI were included (mean age: 60.6 ± 12.2 years; ST-elevation myocardial infarction [STEMI]: 72.8%), of whom 105 (21.6%) were female. Baseline characteristics stratified by sex are summarized in Table 1. Compared with male, female patients were less likely to experience cardiac arrest in a public location (52.1% vs 66.7%, P = .01) and presented less frequently with a shockable rhythm (73.3% vs 85.3%, P = .004). Resuscitation durations were comparable between female and male patients, as were the initial hemodynamic parameters at the time of hospital admission. The median troponin level was higher in female compared with male patients. The antithrombotic management was similar in male and female patients, with a comparable rate of thrombolysis (4.8% vs 2.1%, P = .17) and similar oral P2Y12 inhibitors treatment.
Angiographic and PCI findings
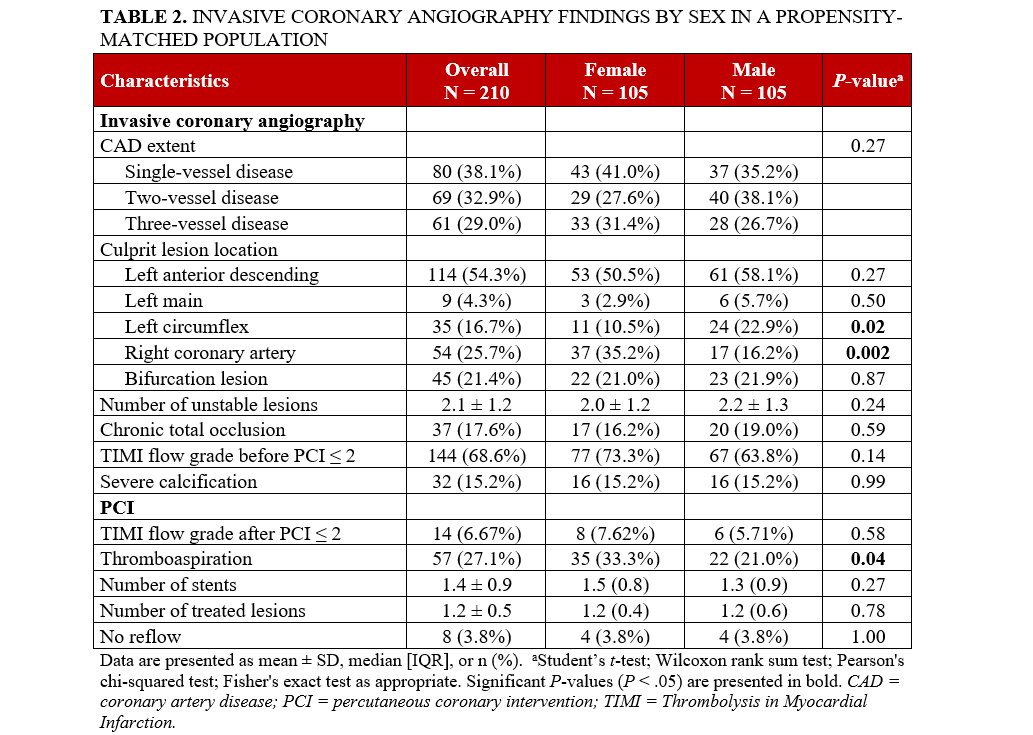
After propensity score matching, 210 patients were included in the analysis (105 female and 105 male patients). The baseline characteristics of the matched population were well balanced (Supplemental Table 1, Supplemental Figure 2). ICA revealed that female patients were significantly more likely to have an RCA culprit lesion than men (35.2% vs 16.2%, P = .002) and less LCx involvement (10.5% vs 22.9%, P = .02). The overall extent of CAD was similar between the 2 groups, with no significant differences observed in the distribution of single or multivessel disease. Other angiographic findings, including the presence of bifurcation lesions, severe calcification, CTO, and a pre-PCI TIMI flow of less than or equal to 2, did not differ significantly by sex (Table 2). Likewise, the number of identified unstable lesions was also similar. In terms of PCI characteristics, thrombus aspiration was more commonly performed in female patients (33.3% vs 21.0%, P = .04), and no differences were found in the number of treated lesions and stents deployed, the presence of a post-PCI TIMI flow of less than or equal to 2, and the occurrence of no-reflow.
Association between sex and outcomes
Regarding in-hospital all-cause death, female patients exhibited a significantly higher rate of event compared with men (51.4% vs 39.6%, P = .03), with female sex being associated with a higher rate of event (odds ratio [OR], 1.61; 95% CI, 1.04-2.49; P = .03) in univariable analysis. However, no association was found after adjustment on potential confounders (OR, 1.43; 95% CI, 0.80-2.55; P = .20). Rates of bleeding, major bleeding, and stent thrombosis were similar between male and female patients (24.3% vs 24.3%, P = .99; 23.3% vs 18.8%, P = .31; and 7.6% vs 7.6%, P = 1.00, respectively), and no associations were found between sex and events after univariable and multivariable analyses (Table 3).
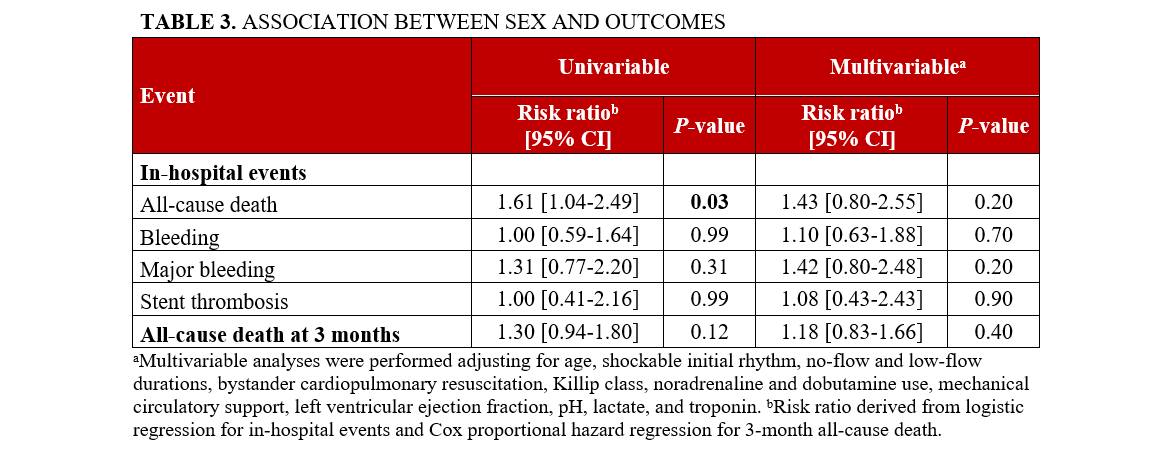
The 3-month all-cause mortality was comparable in both female and male patients (48.5% vs 40.2%, P = .14). No association was found in univariable (hazard ratio [HR], 1.30; 95% CI, 0.94-1.80; P = .12) or multivariable analysis (HR, 1.18; 95% CI, 0.83-1.66; P = .40).
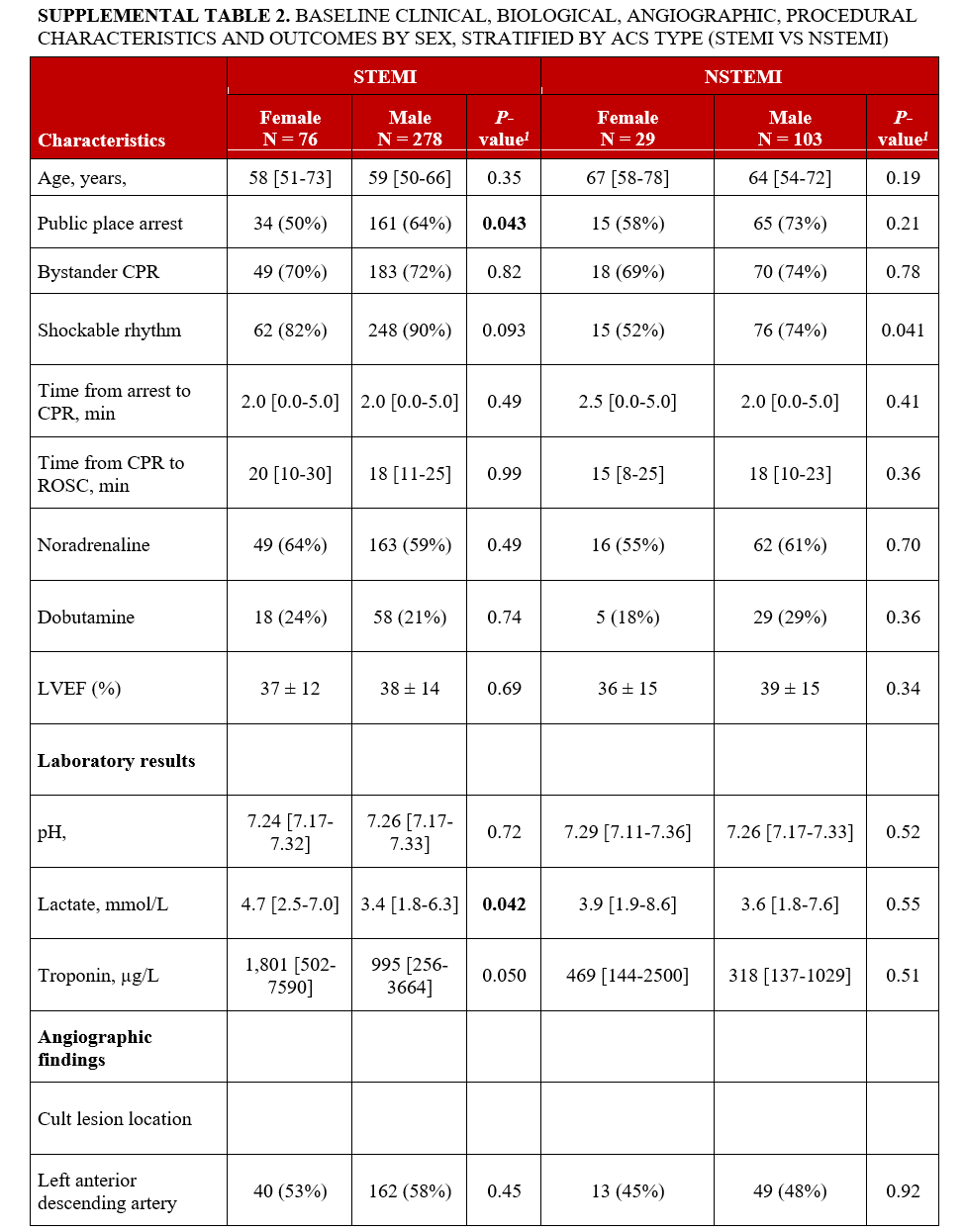
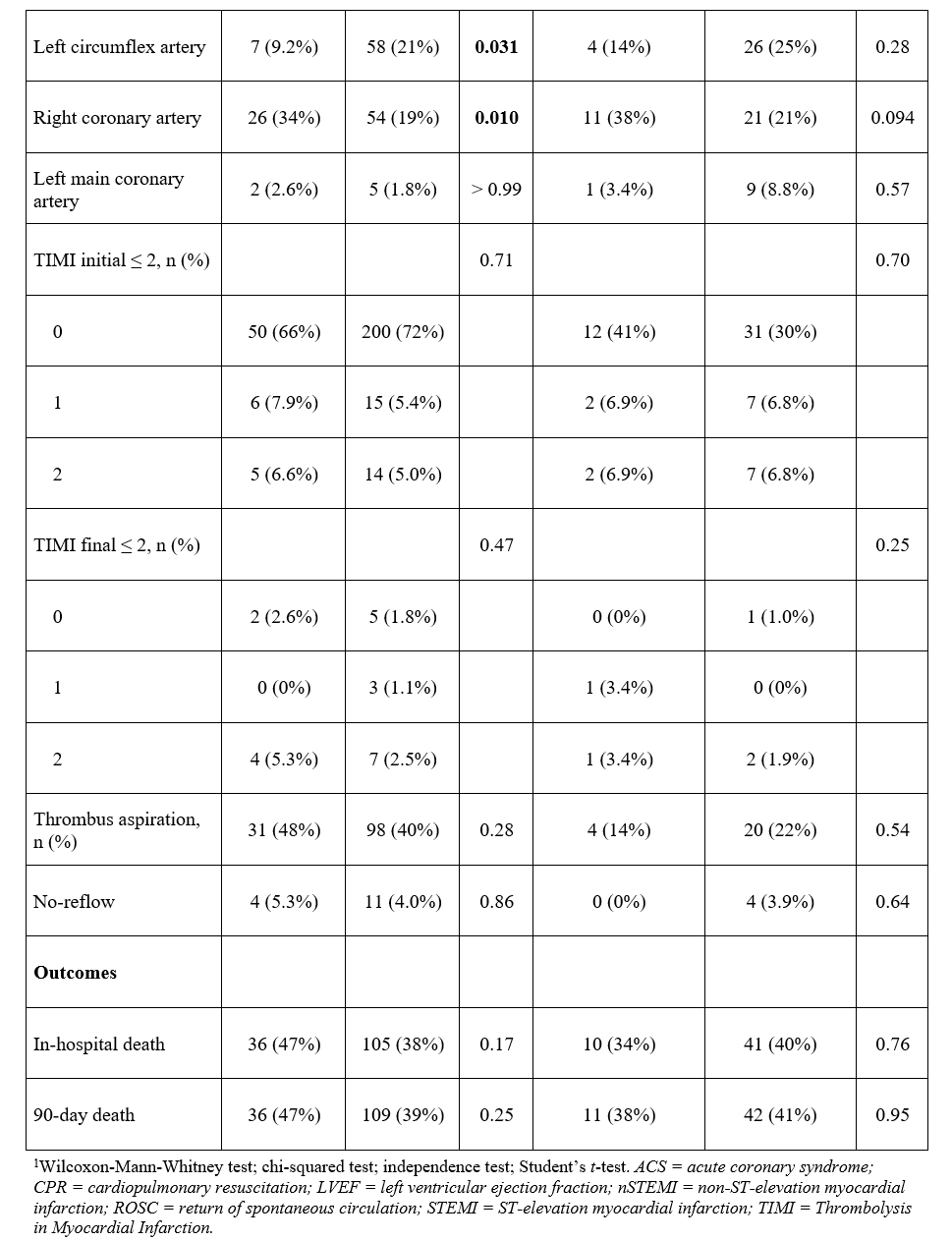
Stratified analysis by ACS type
We performed a stratified analysis according to ACS type (with or without ST-segment elevation). As detailed in Supplemental Table 2, the higher prevalence of RCA culprit lesions in women remained significant in the STEMI subgroup, but not in the non-ST elevation (NSTEMI) subgroup. No sex-related differences were observed in the use of thrombus aspiration or in-hospital and 90-day mortality. In both subgroups, women were less likely to experience OHCA in a public place and had higher lactate levels compared with men. Other clinical, biological, and procedural characteristics were similar between women and men.
Discussion
In this well-characterized cohort of OHCA patients with angiographically confirmed ACS undergoing PCI, no major sex-based differences were observed in the extent or complexity of CAD or in the interventional strategies employed. Aside from minor variations in the culprit artery location and thrombus aspiration use, angiographic and procedural profiles were remarkably similar between male and female patients.
Sex-based disparities in the management of OHCA complicating ACS have been consistently reported in the literature.2-6 Female patients are less likely to undergo ICA following OHCA, despite guideline recommendations promoting early coronary evaluation in these high-risk populations regardless of the sex. Several large registry-based studies have highlighted this disparity, showing significantly lower rates of ICA in female compared with male patients, potentially due to differences in symptom presentation, clinical decision-making biases, or assumptions regarding coronary anatomy.18-20
Among patients who undergo ICA, the rates of PCI are often similar between sexes.7,18,19 Previous studies have suggested that female patients may present more frequently with non-obstructive CAD or less extensive atherosclerotic burden, which could contribute to lower intervention rates.21 However, these studies typically included heterogeneous populations with varying OHCA etiologies or without confirmed ACS, making it difficult to isolate true sex-related differences in coronary anatomy in the setting of OHCA complicating ACS.
In the present study, which focused specifically on OHCA survivors with angiographically confirmed ACS requiring emergent PCI, we observed no significant sex-based differences in the extent or complexity of CAD. The distribution of single-, double-, and triple-vessel disease was similar between male and female patients, and no disparities were noted in the prevalence of bifurcation lesions, CTOs, severe calcification, and impaired pre-PCI TIMI flow. These findings are consistent with prior studies in ACS reporting similar angiographic profiles across sexes.22-24 Angiographic complexity and PCI strategies were broadly similar between sexes. We did observe statistically significant differences in culprit territory: women had more RCA and less LCx involvement. Yet, these pattern-level differences did not translate into disparities in pre- or post-PCI TIMI flow, no-reflow, number of treated lesions/stents, or adjusted outcomes. Stratified analysis by ACS type confirmed these findings, with the excess of RCA culprit lesions in women persisting in STEMI but not NSTEMI. This contrasts with the findings of Lansky et al, who reported a more uniform distribution of culprit lesions by sex, potentially reflecting differences in study populations.22 However, this study only focused on patients with ACS without OHCA.
Similarly, PCI procedural strategies were largely comparable across sexes, with no significant differences in the number of treated lesions or stents deployed. These findings are consistent with those of Savage et al, who reported comparable stent implantation rates following MI in both male and female patients.25 Thrombus aspiration was more frequently performed in female patients; however, this pattern may likely reflect a combination of non-significant trend toward more impaired pre-PCI flow (TIMI < 2: 73.3% vs 63.8%, P = .14) and operator preference, while post-PCI impaired TIMI flow and no-reflow were comparable between sexes. These findings are consistent with the results of Heer et al, who reported comparable PCI success rates between female and male patients following ACS.26
In our cohort, unadjusted analyses initially showed higher all-cause mortality among female patients (Figure). However, after adjustment for baseline characteristics and clinical confounders, sex was no longer independently associated with in-hospital or 3-month mortality. Similarly, rates of bleeding and stent thrombosis did not differ significantly between male and female patients in either univariable or multivariable analyses. These findings align with previous studies suggesting that observed sex-related differences in outcomes may largely reflect disparities in baseline risk and treatment among enrolled patients rather than intrinsic biological differences.2,3 Importantly, all patients in our study underwent emergent angioplasty regardless of sex, underlining a consistent standard of care across groups. This suggests that when timely and optimal care is delivered equally, the prognosis following MI may be similar between male and female patients.
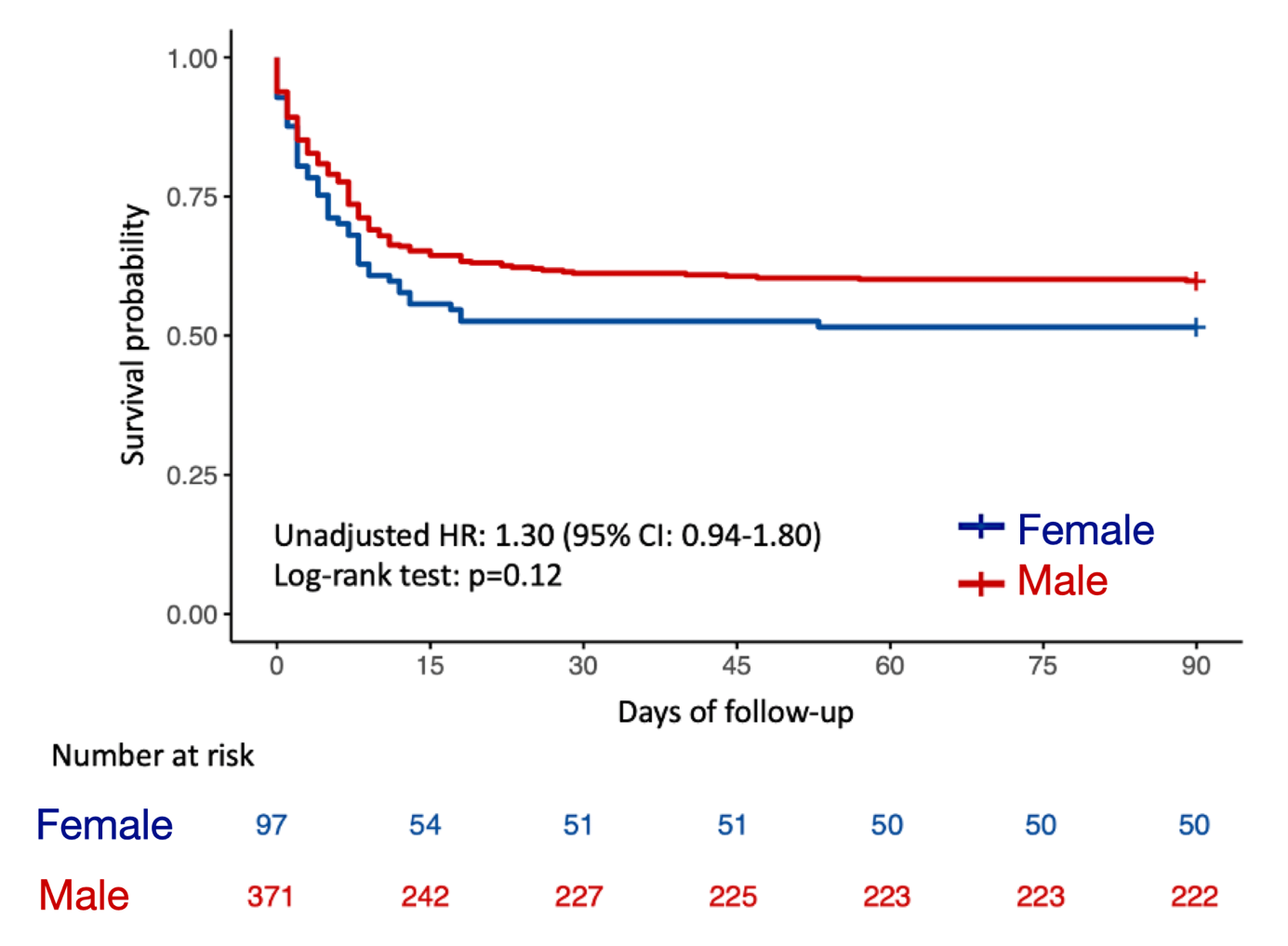
Female (blue line) demonstrated lower unadjusted survival compared with male patients (red line), although the difference was not statistically significant (log-rank: P = .12). HR = hazard ratio.
Limitations
This study has several limitations. First, its retrospective and single-center design may limit the generalizability of our findings. Second, given the modest female sample, power to detect small sex differences is limited. Although we used propensity score matching to adjust for key clinical variables, residual confounding cannot be fully excluded. The functional assessment of coronary lesions (eg, via fractional flow reserve or other physiologic indices) was not systematically performed, limiting our ability to assess whether apparent anatomical similarities translated into comparable ischemic burden.
Conclusions
This is the first study to assess angiographic and PCI characteristics by sex in patients with OHCA complicating ACS and undergoing emergent PCI. No meaningful sex-based differences were observed in the extent or complexity of CAD, nor in PCI strategies or procedural success. These findings indicate that angiographic and procedural factors are unlikely to account for the observed sex differences in outcomes, suggesting that other biologic or systemic factors may play a more significant role.
Affiliations and Disclosures
Manveer Singh, MD, MSc1,2,3; Fabien Picard, MD, PhD1,3,4; Alain Cariou, MD, PhD4,5; Olivier Varenne, MD, PhD1,4; Vincent Pham, MD, MSc1,3,4
Dr Singh and Dr Picard contributed equally to the work.
From the 1Cardiology Department, Cochin Hospital, Assistance Publique-Hôpitaux de Paris, Paris, France; 2Service de Cardiologie, Hospital of Lariboisière, Assistance Publique-Hôpitaux de Paris, Paris, France; 3ARIC Paris Centre, Paris, France; 4Université Paris Cité, Paris, France; 5Medical Intensive Care Unit, Cochin Hospital, Assistance Publique-Hôpitaux de Paris, Paris, France.
Disclosures: Dr Picard reports research, consulting, and speaking fees from Abbott, B. Braun, Biotronik, Boston Scientific, Medtronic, Novartis, Servier, and Sanofi, outside the submitted work. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Vincent Pham, MD, MSc, Cochin Hospital, AP-HP, Université Paris Cité, 27 Rue du Faubourg Saint-Jacques, Paris 75014, France. Email: quang-trung.pham@aphp.fr; X: @picard_fabien
Supplemental Material
References
1. Gräsner JT, Herlitz J, Tjelmeland IBM, et al. European Resuscitation Council Guidelines 2021: epidemiology of cardiac arrest in Europe. Resuscitation. 2021;161:61-79. doi:10.1016/j.resuscitation.2021.02.007
2. Amacher SA, Zimmermann T, Gebert P, et al; Swiss ICU Trial Group. Sex disparities in ICU care and outcomes after cardiac arrest: a Swiss nationwide analysis. Crit Care. 2025;29(1):42. doi:10.1186/s13054-025-05262-5
3. Verghese D, Patlolla SH, Cheungpasitporn W, et al. Sex disparities in management and outcomes of cardiac arrest complicating acute myocardial infarction in the United States. Resuscitation. 2022;172:92-100. doi:10.1016/j.resuscitation.2022.01.024
4. Awad E, Christenson J, Grunau B, Tallon J, Humphries K. Sex differences in out-of-hospital cardiac arrest interventions within the province of British Columbia, Canada. Resuscitation. 2020;148:128-134. doi:10.1016/j.resuscitation.2020.01.016
5. Nehme Z, Andrew E, Bernard S, Smith K. Sex differences in the quality-of-life and functional outcome of cardiac arrest survivors. Resuscitation. 2019;137:21-28. doi:10.1016/j.resuscitation.2019.01.034
6. Wigginton JG, Perman SM, Barr GC, et al. Sex- and gender-specific research priorities in cardiovascular resuscitation: proceedings from the 2014 Academic Emergency Medicine Consensus Conference Cardiovascular Resuscitation Research Workgroup. Acad Emerg Med. 2014;21(12):1343-1349. doi:10.1111/acem.12541
7. Bosson N, Kaji AH, Fang A, et al. Sex differences in survival from out-of-hospital cardiac arrest in the era of regionalized systems and advanced post-resuscitation care. J Am Heart Assoc. 2016;5(9):e004131. doi:10.1161/JAHA.116.004131
8. Karlsson V, Dankiewicz J, Nielsen N, et al. Association of gender to outcome after out-of-hospital cardiac arrest--a report from the International Cardiac Arrest Registry. Crit Care. 2015;19(1):182. doi:10.1186/s13054-015-0904-y
9. Wissenberg M, Hansen CM, Folke F, et al. Survival after out-of-hospital cardiac arrest in relation to sex: a nationwide registry-based study. Resuscitation. 2014;85(9):1212-1218. doi:10.1016/j.resuscitation.2014.06.008
10. Bougouin W, Mustafic H, Marijon E, et al. Gender and survival after sudden cardiac arrest: a systematic review and meta-analysis. Resuscitation. 2015;94:55-60. doi:10.1016/j.resuscitation.2015.06.018
11. Wigginton JG, Pepe PE, Bedolla JP, DeTamble LA, Atkins JM. Sex-related differences in the presentation and outcome of out-of-hospital cardiopulmonary arrest: a multiyear, prospective, population-based study. Crit Care Med. 2002;30(4 Suppl):S131-S136. doi:10.1097/00003246-200204001-00002
12. Blom MT, Oving I, Berdowski J, van Valkengoed IGM, Bardai A, Tan HL. Women have lower chances than men to be resuscitated and survive out-of-hospital cardiac arrest. Eur Heart J. 2019;40(47):3824-3834. doi:10.1093/eurheartj/ehz297
13. Böckler B, Preisner A, Bathe J, et al. Gender-related differences in adults concerning frequency, survival and treatment quality after out-of-hospital cardiac arrest (OHCA): an observational cohort study from the German resuscitation registry. Resuscitation. 2024;194:110060. doi:10.1016/j.resuscitation.2023.110060
14. Nolan JP, Sandroni C, Böttiger BW, et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care. Intensive Care Med. 2021;47(4):369-421. doi:10.1007/s00134-021-06368-4
15. Nolan JP, Soar J, Cariou A, et al; European Resuscitation Council; European Society of Intensive Care Medicine. European Resuscitation Council and European Society of Intensive Care Medicine 2015 guidelines for post-resuscitation care. Intensive Care Med. 2015;41(12):2039-2056. doi:10.1007/s00134-015-4051-3
16. Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation. 2011;123(23):2736-2747. doi:10.1161/CIRCULATIONAHA.110.009449
17. Garcia-Garcia HM, McFadden EP, Farb A, et al; Academic Research Consortium. Standardized end point definitions for coronary intervention trials: the Academic Research Consortium-2 consensus document. Circulation. 2018;137(24):2635-2650. doi:10.1161/CIRCULATIONAHA.117.029289
18. Bougouin W, Dumas F, Marijon E, et al. Gender differences in early invasive strategy after cardiac arrest: insights from the PROCAT registry. Resuscitation. 2017;114:7-13. doi:10.1016/j.resuscitation.2017.02.005
19. Winther-Jensen M, Hassager C, Kjaergaard J, et al. Women have a worse prognosis and undergo fewer coronary angiographies after out-of-hospital cardiac arrest than men. Eur Heart J Acute Cardiovasc Care. 2018;7(5):414-422. doi:10.1177/2048872617696368
20. Winther-Jensen M, Kjaergaard J, Wanscher M, et al. No difference in mortality between men and women after out-of-hospital cardiac arrest. Resuscitation. 2015;96:78-84. doi:10.1016/j.resuscitation.2015.06.030
21. Lindgren E, Covaciu L, Smekal D, et al. Gender differences in utilization of coronary angiography and angiographic findings after out-of-hospital cardiac arrest: a registry study. Resuscitation. 2019;143:189-195. doi:10.1016/j.resuscitation.2019.07.015
22. Lansky AJ, Ng VG, Maehara A, et al. Gender and the extent of coronary atherosclerosis, plaque composition, and clinical outcomes in acute coronary syndromes. JACC Cardiovasc Imaging. 2012;5(3 Suppl):S62-S72. doi:10.1016/j.jcmg.2012.02.003
23. Chandrasekhar J, Mehran R. Sex-based differences in acute coronary syndromes: insights from invasive and noninvasive coronary technologies. JACC Cardiovasc Imaging. 2016;9(4):451-464. doi:10.1016/j.jcmg.2016.02.004
24. Seegers LM, Araki M, Nakajima A, et al. Sex Differences in culprit plaque characteristics among different age groups in patients with acute coronary syndromes. Circ Cardiovasc Interv. 2022;15(6):e011612. doi:10.1161/CIRCINTERVENTIONS.121.011612
25. Savage ML, Hay K, Vollbon W, et al. Differences between sexes in STEMI treatment and outcomes with contemporary primary PCI. Catheter Cardiovasc Interv. 2024;104(5):934-944. doi:10.1002/ccd.31206
26. Heer T, Hochadel M, Schmidt K, et al. Sex differences in percutaneous coronary intervention-insights from the coronary angiography and PCI registry of the German Society of Cardiology. J Am Heart Assoc. 2017;6(3):e004972. doi:10.1161/JAHA.116.004972













