


Sex Specificities of Patients Undergoing Coronary Procedures and Experiencing Transradial Approach Failures
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Objectives. Failed transradial approach (TRA) in patients undergoing percutaneous coronary procedures is associated with higher rates of vascular complications. While female sex is associated with an increased risk of failed TRA, it is unknown if females are also exposed to an increased risk of adverse events after access crossover. The authors compared the outcomes of males and females experiencing crossover following a failed TRA.
Methods. The REPEAT study prospectively enrolled patients undergoing coronary procedures through TRA with access failure. In this subanalysis, patients were stratified according to sex. Propensity score matching for major confounders was used to generate comparable groups. The primary outcome was a composite of vascular complication and significant bleeding.
Results. Of 462 patients experiencing TRA failure, 245 were male and 217 female. Female patients were older and showed fewer comorbidities. TRA failure was more commonly related to radial tortuosity in females and subclavian tortuosity in males. After propensity score matching, 123 pairs were selected. Females showed higher rates of femoral crossover compared with males, in whom a contralateral radial access is mostly preferred. The incidence of the primary outcome was comparable between the 2 groups (males: 8.1% vs females: 12.2%; odds ratio [OR], 1.57; 95% CI, 0.68-3.64; P = .294). Consistent results were evident in a sensitivity analysis on patients undergoing crossover to femoral access (males: 14.5% vs females: 13.0%; OR, 0.8; 8 95% CI, 0.33-2.33; P = .805).
Conclusions. In patients experiencing a failed TRA, no statistically significant differences were evident in terms of vascular complications or bleeding between females and males.
Introduction
The transradial approach (TRA) represents the standard vascular access in patients undergoing coronary angiography and/or percutaneous coronary interventions (PCI) because of its higher safety profile compared with the femoral approach.1,2 Despite the fact that its use has decreased significantly over the years as operators’ experience increases, TRA failure still ranges between 2.5% and 5.0% in unselected patients undergoing a primary radial access.3-5 This complication is not trivial, and evidence has been published showing that subjects who experience a TRA failure are exposed to an increased risk of vascular complications, periprocedural bleedings, and even mortality.5-8 Previous investigations have shown that female patients have an increased risk of TRA failure and crossover to femoral access, probably due to a higher prevalence of frailty factors and anatomical obstacles.4,9 However, it remains unknown if the anatomical and clinical features of female patients also expose them to an increased risk of periprocedural complications after TRA failure has occurred, as well as if specific therapeutic actions should be taken accordingly or not. The aims of this study were to compare the risk of adverse vascular events between male and female patients experiencing access crossover because of a failed primary TRA.
Methods
Study design
This is a non-prespecified subanalysis of “The Radial accEss Crossover for PErcutaneous Coronary Procedures And outcome” (REPEAT) study (NCT 05340998).6 The study design and methods have been previously described. Briefly, the REPEAT study prospectively enrolled consecutive patients undergoing coronary angiography and/or PCI with a transradial approach (TRA) in 10 Italian centers between July 2022 and January 2025. The enrollment was performed in a 2:1 fashion including patients with successful and failed (crossover) first TRA.
All procedures were performed by experienced operators. The choice of the modality of puncture as well as the site of the first radial attempt (right or left) was left to the operator’s discretion. Main exclusion criteria were age younger than 18 years, hemodynamic instability or need for mechanical support, primary non-radial or distal radial access, and procedures requiring more than 1 vascular access. All patients signed a dedicated informed consent. The study was approved by the Ethical Committees of each enrolling center and conducted according to the principles of the Declaration of Helsinki.
Study objectives and population
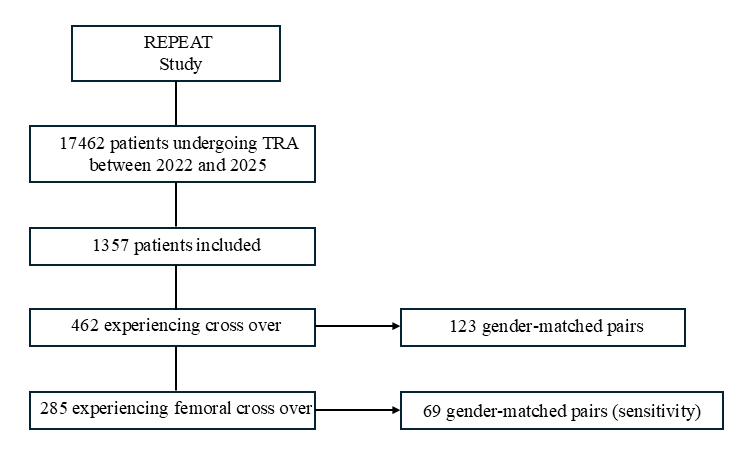
The aims of this study were to assess the clinical outcomes of patients experiencing crossover according to sex. Therefore, for the purposes of the present research, only those subjects experiencing a first failed TRA in the original REPEAT study were included. Comparable groups were generated using propensity score matching according to sex, and clinical outcomes were compared. A sensitivity analysis was performed, which included only patients who underwent femoral crossover as final vascular access. The study flow chart has been synthesized in Figure 1.
Clinical outcomes
All clinical endpoints were systematically assessed 24 hours following the procedures. The primary outcome was a composite of any vascular complication (any vascular damage clinically or instrumentally documented as vessel perforation, arteriovenous fistula, pseudoaneurysm, arterial dissection, retroperitoneal hematoma, compartmental syndrome, or other vascular complications requiring surgery) and significant bleedings, as defined by the Bleeding Academic Research Consortium (BARC) recommendations (grade 2 or 3).10 The secondary outcomes were the isolated composers of the primary one and the occurrence of any bleeding.
Statistics
Categorical variables were described as row number and frequencies, continuous variables as median and interquartile ranges (IQR). Normal distribution of continuous variables was tested with the Shapiro-Wilk test. Categorical variables were compared with the chi-squared test, and continuous variables with the Mann-Whitney U test. Propensity score matching was used to generate comparable groups based on sex.
Starting from subjects experiencing any type of crossover (either radial or femoral) following a first failed TRA (N = 462), a multivariate logistic regression model was designed using female sex as dependent variable and the following confounders as independent variables: age, body mass index (BMI), hypertension, diabetes, dyslipidemia, smoking status, chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), peripheral artery disease (PAD), previous cerebrovascular accident (CVA), previous myocardial infarction (MI), previous coronary angiography or PCI, previous coronary artery bypass grafting (CABG), preprocedural international normalized ratio, preprocedural hemoglobin, aspirin therapy, P2Y12 therapy, oral anticoagulation (OAC), acute coronary syndrome (ACS) at the time of inclusion, ST elevation (STEMI) or non-ST elevation MI (NSTEMI), and the type of procedure (coronary angiography or PCI).
Following, propensity score was calculated and greedy: 1:1 nearest-neighbor matching with no replacement, and a caliper set at 0.2 of the standard deviation of the logit of the propensity score was performed to generate comparable cohorts. The balance between the matched groups was checked calculating the standard mean difference of the confounding variables. A dedicated sensitivity analysis was performed with a multivariate model adjusted for variables not included in the matching process (heparin dose, femoral access, procedural time) and robust standard errors clustered at center-level. Similarly, starting from subjects undergoing femoral crossover (n = 285), the same strategy was applied as a sensitivity analysis. Clinical outcomes were assessed between the matched cohorts using univariate logistic regression and reported as odds ratio (OR) and 95% confidence intervals (CI). Statistical significance was set for 2-tailed P-values of less than or equal to 0.05. All analyses were conducted with STATA 16 (Stata Corp).
Results
Baseline features of patients experiencing first TRA failure according to sex
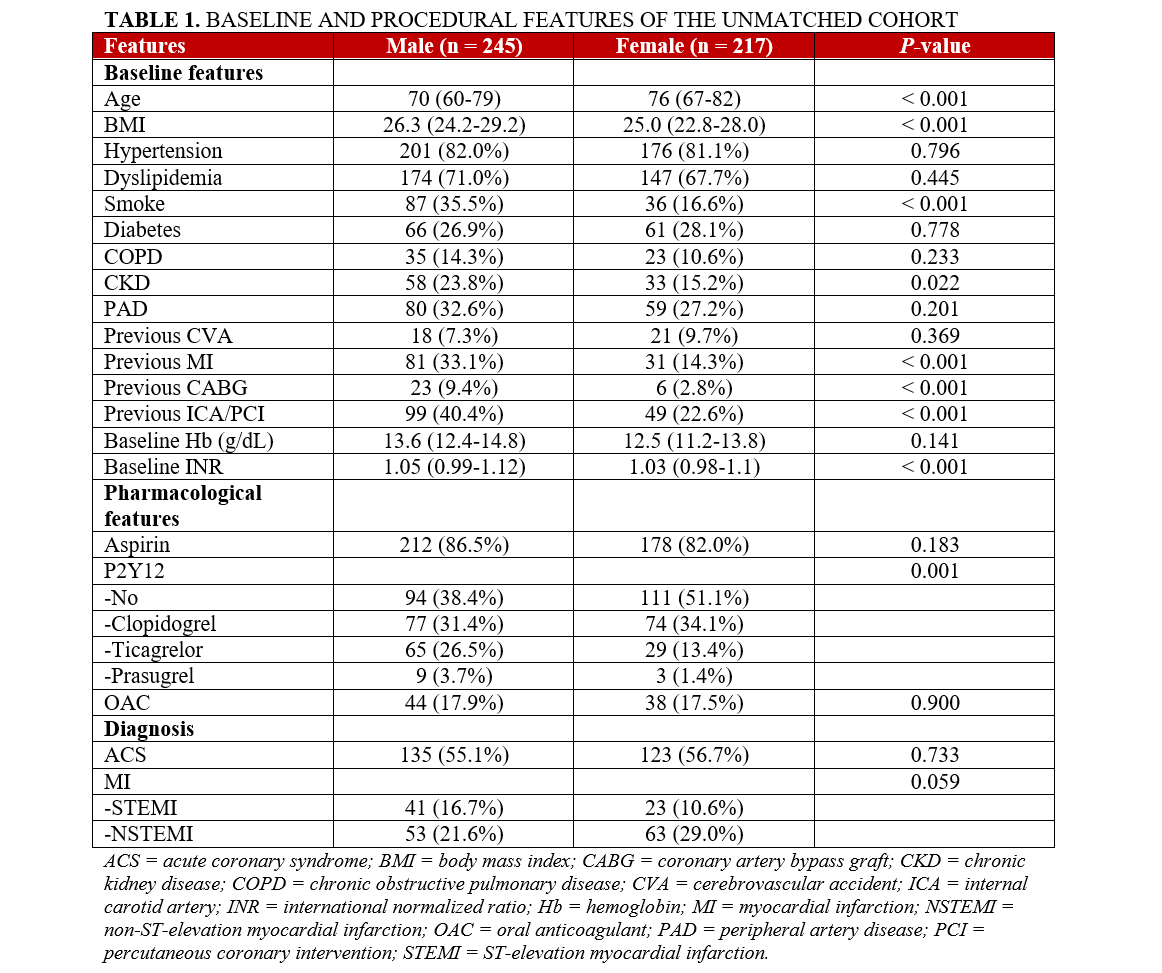
Within the 462 patients experiencing first TRA failure, 245 (53%) were male and 217 (47%) were female. The female patients were significantly older (P < .001) and presented a lower prevalence of major risk factors such as lower BMI (P < .001), smoking status (P < .001), CKD (P = .022), previous MI (P < .001), previous CABG (P < .001), and previous coronary procedures (P < .001). Regarding pharmacological treatment, female patients were more rarely treated with dual antiplatelet therapy and more often with clopidogrel rather than with strong P2Y12 inhibitors. A tendency towards higher rates of NSTEMI compared with STEMI was evident in female patients compared with males (P = .059). These results are shown in Table 1.
Procedural features and causes of failed first TRA across the sexes
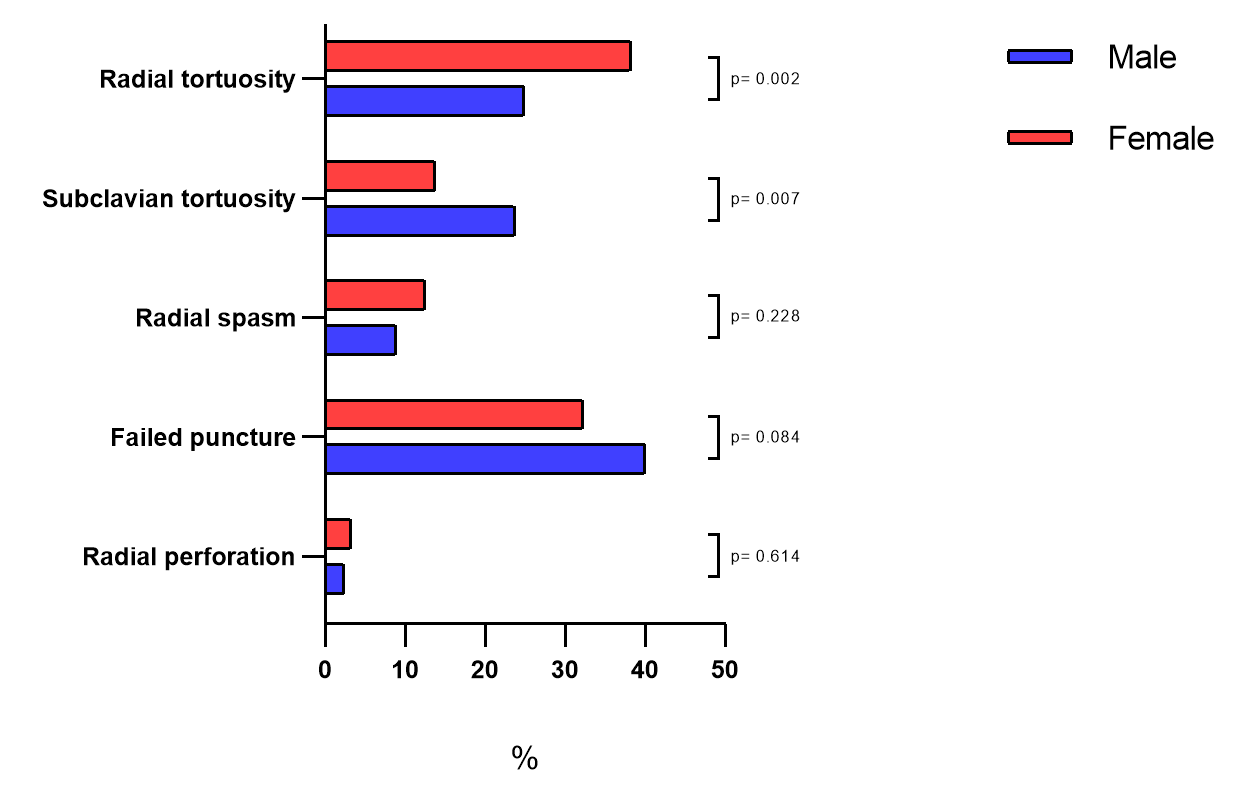
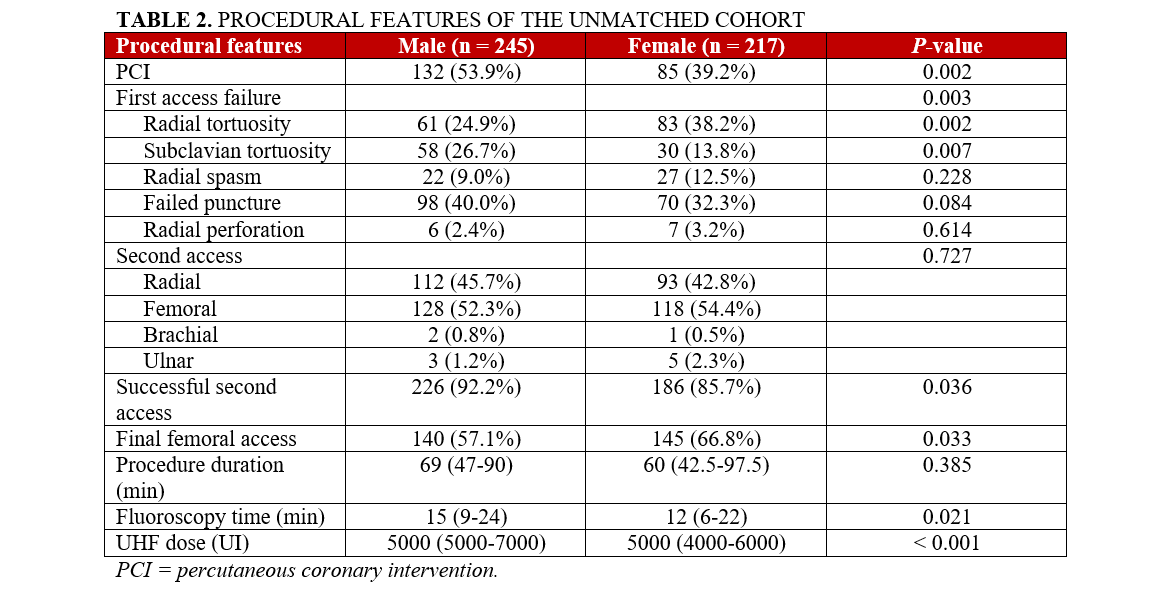
In terms of procedural characteristics, female patients were less frequently treated with PCI (P = .002). Radial tortuosity caused first TRA failure in 61 males (24.9%) and 83 females (38.2%) (P = .002). Alternatively, subclavian tortuosity was more common in male patients (58 [3.7%]) than in females (30 [13.8%]). The other causes of first TRA failure (radial spasm, failed puncture attempt, and radial perforation) were comparable between the 2 groups (Figure 2). The second vascular access was more frequently successful in male patients than in females (226 [92.2%] vs 186 [85.7%]; P = .036). A final femoral approach was more often used in female patients than in males (145 [66.8%] vs 140 [57.1%]; P = .033). These results are reported in Table 2.
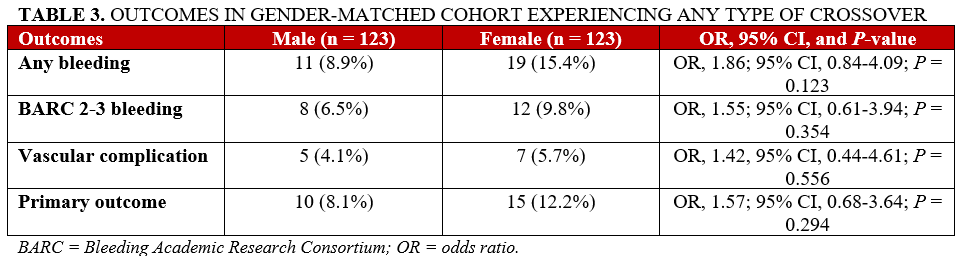
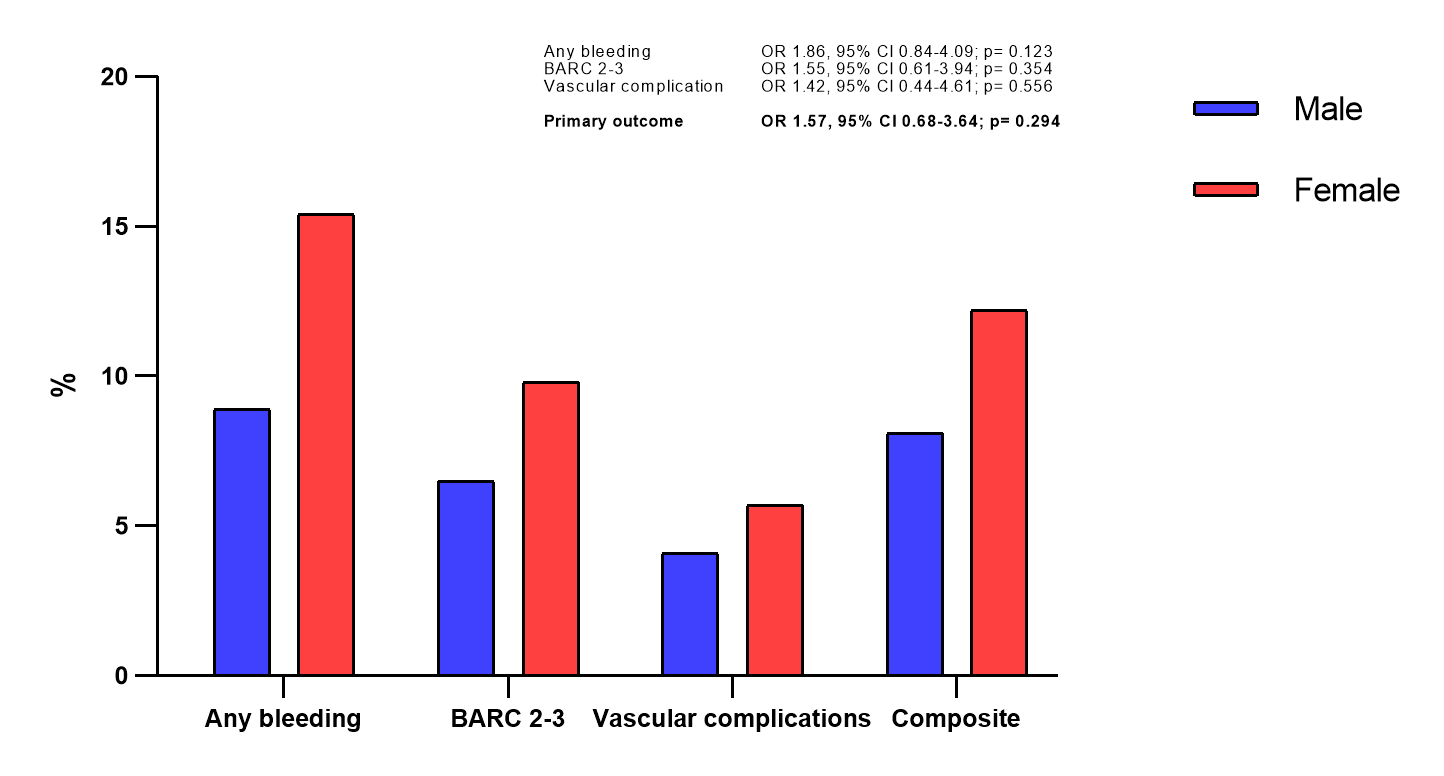
Clinical outcomes in patients experiencing any type of crossover
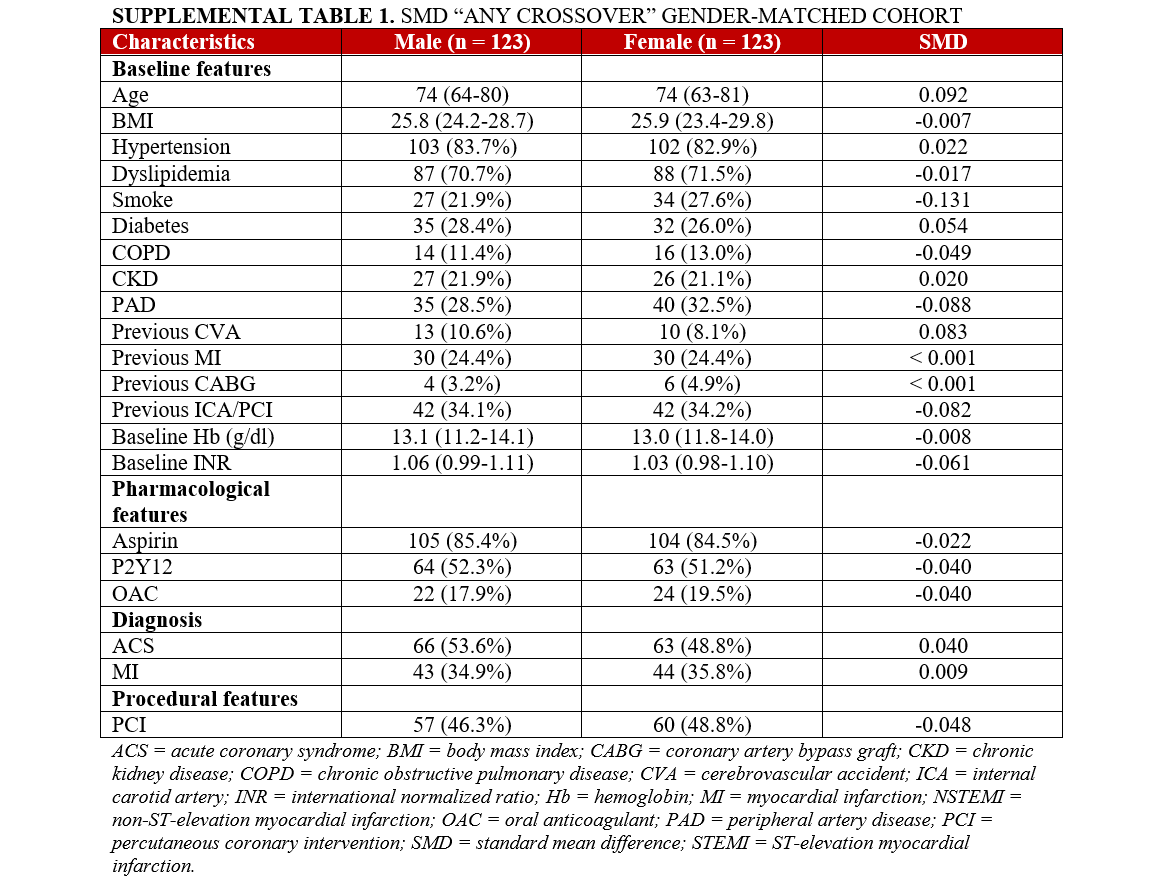
After propensity score matching, 123 matched pairs of male and female patients experiencing any type of crossover (either femoral or not) were selected. An acceptable balance was evident for all the confounders used for the matching generation (Supplemental Table 1). Femoral access represented the final effective vascular route in 53.7% of male patients and 67.5% of female patients (P = .027). Overall, the incidence of the primary outcome of any vascular complication and BARC 2-3 bleeding was comparable between the male and female groups (10 [8.1%] vs 15 [12.2%]; OR, 1.57; 95% CI, 0.68-3.64; P = .294). This finding was confirmed after adjusting for residual confounders/enrolling center (OR, 1.40; 95% CI, 0.70-2.78) and after investigating the interaction between the femoral access and the sex (p-int = .637). Similar results were evident for the secondary outcomes: any bleeding (11 males [8.9%] vs 19 females [15.4%]; OR, 1.86; 95% CI, 0.84-4.09; P = .123), BARC 2-3 bleeding (8 males [6.5%] vs 12 females [9.8%]; OR, 1.55; 95% CI, 0.61-3.94; P = .354), vascular complications (8.1% male vs 12.2%, female; OR 1.57; 95% CI, 0.68-3.6; P = .294). These results are shown in Table 3 and Figure 3.
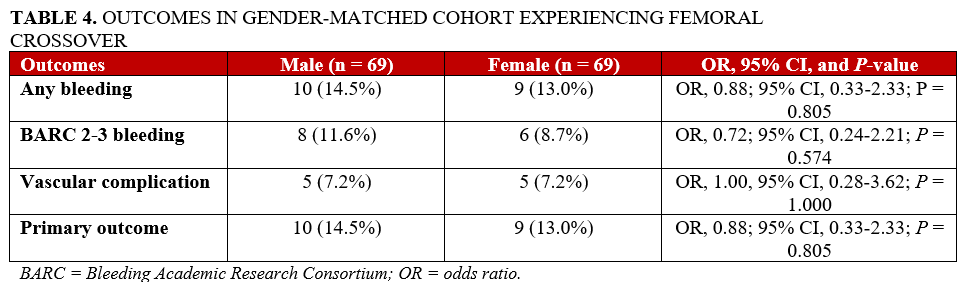
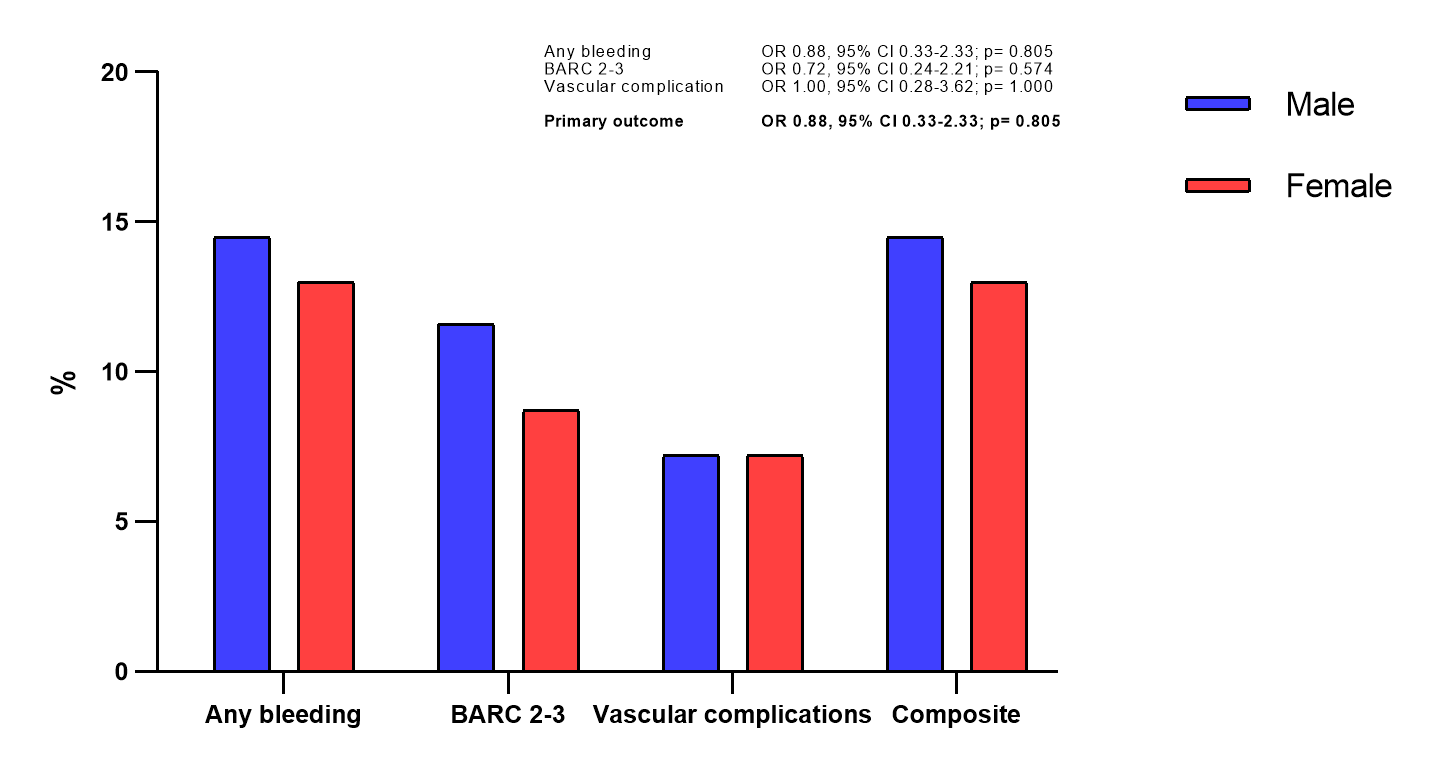
Sensitivity analysis in patients experiencing femoral crossover
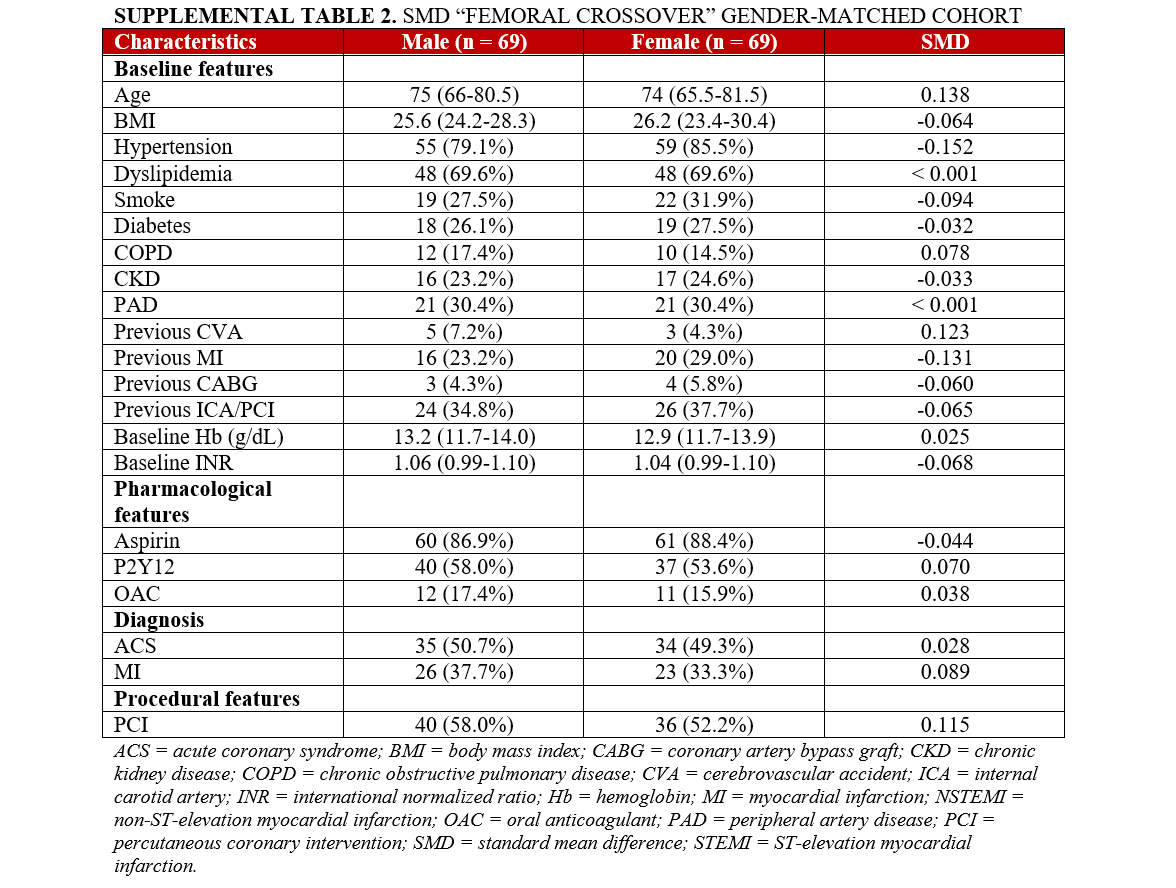
From the patients who underwent femoral procedures following TRA failure, 69 matched pairs of males and females were selected (118 as second access attempt and 20 as third access attempt). The balance between the confounders used for matching is reported in Supplemental Table 2. The risk of the primary outcome was comparable between the 2 groups (10 males [14.5%] vs 9 females [13.0%]; OR, 0.88; 95% CI, 0.33-2.33; P = .805). Similarly, no differences were evident for the secondary outcomes. These data are shown in Table 4 and Figure 4.
Discussion
According to our findings, of patients undergoing coronary angiography or PCI who experience a failed first TRA, female sex was not associated with an increased risk of vascular complications or bleedings. These results were confirmed even when the analysis was restricted only to patients who underwent a femoral crossover. To the best of our knowledge, this is the first study specifically focusing on the sex specificities of patients experiencing a first radial access failure.
TRA is the standard method of performing coronary angiography and PCI because of its capacity to reduce periprocedural adverse events.1,2 The association between post-PCI vascular complications or bleedings and strong endpoints such as mortality has been largely demonstrated,5,11 and recent evidence has shown that the progressive implementation of TRA in clinical practice has significantly contributed to the improvement of outcomes of all-comer patients undergoing PCI.12 Despite this, the risk of access-related complications has not been abolished and they still occur in a significant proportion of patients, probably because of the increasing clinical complexity of patients eligible for PCI and the decreasing operator experience with femoral access.13
The higher risk of vascular complications and bleedings in female patients has been often reported in studies comparing radial and femoral approaches for PCI.9,14 However, there is uncertainty regarding the mechanisms underlying this risk. Specifically, several previous investigations (including the REPEAT study) have reported that the rates of a first TRA failure are increased in female subjects, with a higher occurrence of crossovers to femoral access.4,6,15,16 Therefore, it is unclear if female sex is associated per se with worse access-related outcomes, or if those previous reports reflected the increased risk of radial failures in these patients. This issue is further complicated by the fact that previous studies investigating sex disparities in patients hospitalized for chronic or acute coronary syndromes have shown that women are generally exposed to several other detrimental outcomes as a result of significant differences in terms of treatment modalities and baseline risk profiles compared with men.17,18
In our study, when female and male patients experiencing a failed TRA were matched and compared, the risk of vascular complications and access-related bleedings was similar. Considering that no investigations have been previously conducted on this topic, comparing our results with the available literature may be challenging. In a previous registry by Stehli et al, female patients with ACS were exposed to a significantly increased risk of 30-day major bleedings, regardless of the use of the radial approach (OR, 1.38; 95% CI; 1.05-1.81; P = .019).16 Notably, no data were available regarding the sources of those events (vascular or not) in that research.
Different results were reported in a dedicated subanalysis of the “Radial Vs femorAL access for coronary intervention” (RIVAL) trial.9 In that study, while women showed an overall increased risk of major vascular complications (HR, 2.39; 95% CI, 1.76-3.2; P < .001), the interaction analyses between vascular access (radial vs femoral) and sex (male vs female) were all negative (RIVAL-major bleedings: p-int. = .748; major vascular complications: p-int. = .092). Similar results were published from a substudy of the “Minimizing Adverse Haemorrhagic Events by TRansradial Access Site and Systemic Implementation of angio X” (MATRIX) trial. Again, while women were exposed to an increased risk of access-site complications, no interaction was evident for major endpoints including BARC 3-5 bleedings (p-int. = .45).14 The results coming from these 2 trials may suggest that the vascular route, instead of sex, could be the main determinant of the risk for access-related impaired outcomes. While women may be exposed to an increased risk of TRA failure, they do not face higher vascular complications rates when compared with males who experience a primary access failure as well. Although this corroborates our findings, it must be noted that none of these studies were specifically designed to analyze patients experiencing crossovers and, therefore, this conclusion can be considered only speculative.
Overall, our results claim for a cautious approach to the estimation of the risk of vascular access complications across the 2 sexes. While women may not be exposed per se to an increased risk of adverse periprocedural events, the higher risk of TRA failure in this group has been widely reported.6,9 Therefore, significant efforts should be spent on avoiding TRA failure to reduce sex-specific impaired outcomes. Despite not being specifically investigated in the REPEAT study, several strategies such as preprocedural ultrasound evaluation of the radial artery, routine use of spasmolytic medications, and the avoidance of anticoagulation before accessing the ascending aorta may all be useful for reducing the rates of TRA failure and the possibly related vascular and bleeding risks.
Limitations
Besides those present in the original REPEAT study, our work has several other major limitations that should be accounted for. First, the reduced sample size of our cohort has surely influenced the results. Specifically, while the overall effect estimates were all negative, female patients in the matched cohorts experienced a numerically higher number of events. Therefore, underpowering may have contributed to our findings, which should be considered only as hypothesis-generating. For the same reason, we could not provide any reliable analysis between the relationship of the number and subtypes of crossover attempts and the risk for adverse events. Second, no clinical follow-up was available, preventing us from accessing sex-specific relationships between TRA failure and strong clinical endpoints such as mortality. Third, despite effective balancing between the various confounders being achieved, residual bias related to risk-profile heterogeneity cannot be completely ruled out, especially when working with limited samples. Fourth, the assessment of vascular complications at 24 hours prevented us from detecting later events, limiting the validity of our findings. Eventually, several other factors that may influence the rates of vascular complications such as sheath sizes, number of puncture attempts, and use of intravascular ultrasound or closure devices were not collected in our registry, which hinders the generalizability of our results.
Conclusions
In our study, no statistically significant differences in terms of vascular complications and access site-related bleedings were evident between female and male patients undergoing coronary angiography or PCI and experiencing a first TRA failure. Further and larger studies are needed to explore the sex specificities of patients experiencing crossover to a second vascular access following a failed initial radial attempt.
Affiliations and Disclosures
Carmine Musto, MD, PhD1; Luca Paolucci, MD2; Giulia Nardi, MD3; Enrico Romagnoli, MD, PhD4; Flavia Belloni, MD5; Giovanni Farraiuoli, MD1; Giuseppe Talanas, MD6; Attilio Placanica, MD, PhD1; Massimo Mancone, MD, PhD7; Enrico Occhiuzzi, MD8; Francesco De Felice, MD2; Alessandro Sciahbasi, MD9
From the 1Cardiology Unit, Ospedale S. Giovanni Evangelista, Tivoli, Italy; 2Division of Interventional Cardiology, Azienda Ospedaliera S. Camillo Forlanini, Rome, Italy; 3Division of Interventional Cardiology, Hospital Clinico San Carlos, Madrid, Spain; 4Department of Cardiovascular Sciences, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy; 5Division of Cardiology, Ospedale Santo Spirito in Saxia, Rome, Italy; 6Clinical and Interventional Cardiology Unit, Sassari University Hospital, Sassari, Italy; 7Department of Clinical, Internal, Anesthesiology and Cardiovascular Sciences, Umberto I Hospital, Sapienza University of Rome, Italy; 8Interventional Cardiology Unit, San Filippo and Nicola Hospital, Avezzano, Italy; 9Interventional Cardiology Unit, Sandro Pertini Hospital, Rome, Italy.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Carmine Musto, MD, PhD, Cardiology Unit, Ospedale S. Giovanni Evangelista, Via Antonio Parrozzani, 3, Tivoli 00019, Italy. Email: cmusto@hotmail.it
References
1. Valgimigli M, Gagnor A, Calabró P, et al; MATRIX Investigators. Radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: a randomised multicentre trial. Lancet. 2015;385(9986):2465-2476. doi:10.1016/S0140-6736(15)60292-6
2. Jolly SS, Yusuf S, Cairns J, et al; RIVAL trial group. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011;377(9775):1409-1420. doi:10.1016/S0140-6736(11)60404-2
3. Gragnano F, Jolly SS, Mehta SR, et al. Prediction of radial crossover in acute coronary syndromes: derivation and validation of the MATRIX score. EuroIntervention. 2021;17(12):e971-e980. doi:10.4244/EIJ-D-21-00441
4. Abdelaal E, Brousseau-Provencher C, Montminy S, et al; Interventional Cardiologists at Quebec Heart-Lung Institute. Risk score, causes, and clinical impact of failure of transradial approach for percutaneous coronary interventions. JACC Cardiovasc Interv. 2013;6(11):1129-1137. doi:10.1016/j.jcin.2013.05.019
5. Sampath-Kumar R, Mahmud E, Korkmaz K, et al. Patient characteristics and outcomes of radial to femoral access-site crossover. J Soc Cardiovasc Angiogr Interv. 2025;4(1):102450. doi:10.1016/j.jscai.2024.102450
6. Sciahbasi A, Cristiano E, Romagnoli E, et al. Radial access crossover for percutaneous coronary procedures and outcome: the REPEAT study. Int J Cardiol. 2025;437:133523. doi:10.1016/j.ijcard.2025.133523
7. Abdelaal E, MacHaalany J, Plourde G, et al. Prediction and impact of failure of transradial approach for primary percutaneous coronary intervention. Heart. 2016;102(12):919-925. doi:10.1136/heartjnl-2015-308371
8. Tornyos D, Lukács R, Jánosi A, Komócsi A. Prognosis impact and prediction of trans-radial access failure in patients with STEMI, a nationwide observational study. Am J Cardiol. 2024;220:23-32. doi:10.1016/j.amjcard.2024.03.016
9. Pandie S, Mehta SR, Cantor WJ, et al. Radial versus femoral access for coronary angiography/intervention in women with acute coronary syndromes: insights from the RIVAL trial (Radial Vs femorAL access for coronary intervention). JACC Cardiovasc Interv. 2015;8(4):505-512. doi:10.1016/j.jcin.2014.11.017
10. Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation. 2011;123(23):2736-2747. doi:10.1161/CIRCULATIONAHA.110.009449
11. Applegate R, Sacrinty M, Little W, Gandhi S, Kutcher M, Santos R. Prognostic implications of vascular complications following PCI. Catheter Cardiovasc Interv. 2009;74(1):64-73. doi:10.1002/ccd.21960
12. Fazel R, Rao SV, Cohen DJ, et al. Radial vs femoral access for percutaneous coronary intervention: temporal trends and outcomes in the USA. Eur Heart J. 2026;47(5):625-636. doi:10.1093/eurheartj/ehaf426
13. Kopin D, Seth M, Sukul D, et al. Primary and secondary vascular access site complications associated with percutaneous coronary intervention: insights from the BMC2 registry. JACC Cardiovasc Interv. 2019;12(22):2247-2256. doi:10.1016/j.jcin.2019.05.051
14. Gargiulo G, Ariotti S, Vranckx P, et al. Impact of sex on comparative outcomes of radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: data from the randomized MATRIX-access trial. JACC Cardiovasc Interv. 2018;11(1):36-50. doi:10.1016/j.jcin.2017.09.014
15. Dang D, Dowling C, Zaman S, Cameron J, Kuhn L. Predictors of radial to femoral artery crossover during primary percutaneous coronary intervention: a systematic review and meta-analysis. Heart Lung Circ. 2021;30(Suppl 3):S318. doi:10.1016/j.hlc.2021.06.498
16. Stehli J, Duffy SJ, Koh Y, et al. Sex differences in radial access for percutaneous coronary intervention in acute coronary syndrome are independent of body size. Heart Lung Circ. 2021;30(1):108-114. doi:10.1016/j.hlc.2020.06.023
17. Lempereur M, Magne J, Cornelis K, et al. Impact of gender difference in hospital outcomes following percutaneous coronary intervention. Results of the Belgian Working Group on Interventional Cardiology (BWGIC) registry. EuroIntervention. 2016;12(2):e216-e223. doi:10.4244/EIJY14M12_11
18. Kim SR, Bae S, Lee JY, et al. Gender disparities in prevalence by diagnostic criteria, treatment and mortality of newly diagnosed acute myocardial infarction in Korean adults. Sci Rep. 2023;13(1):4120. doi:10.1038/s41598-023-31014-y y













