Left-Sided Inferior Vena Cava: An Unusual Obstacle to Leadless Pacemaker Implantation
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00030. Epub February 26, 2026.
A 68-year-old man was admitted for intermittent high grade atrioventricular block. Leadless pacemaker implantation was planned.
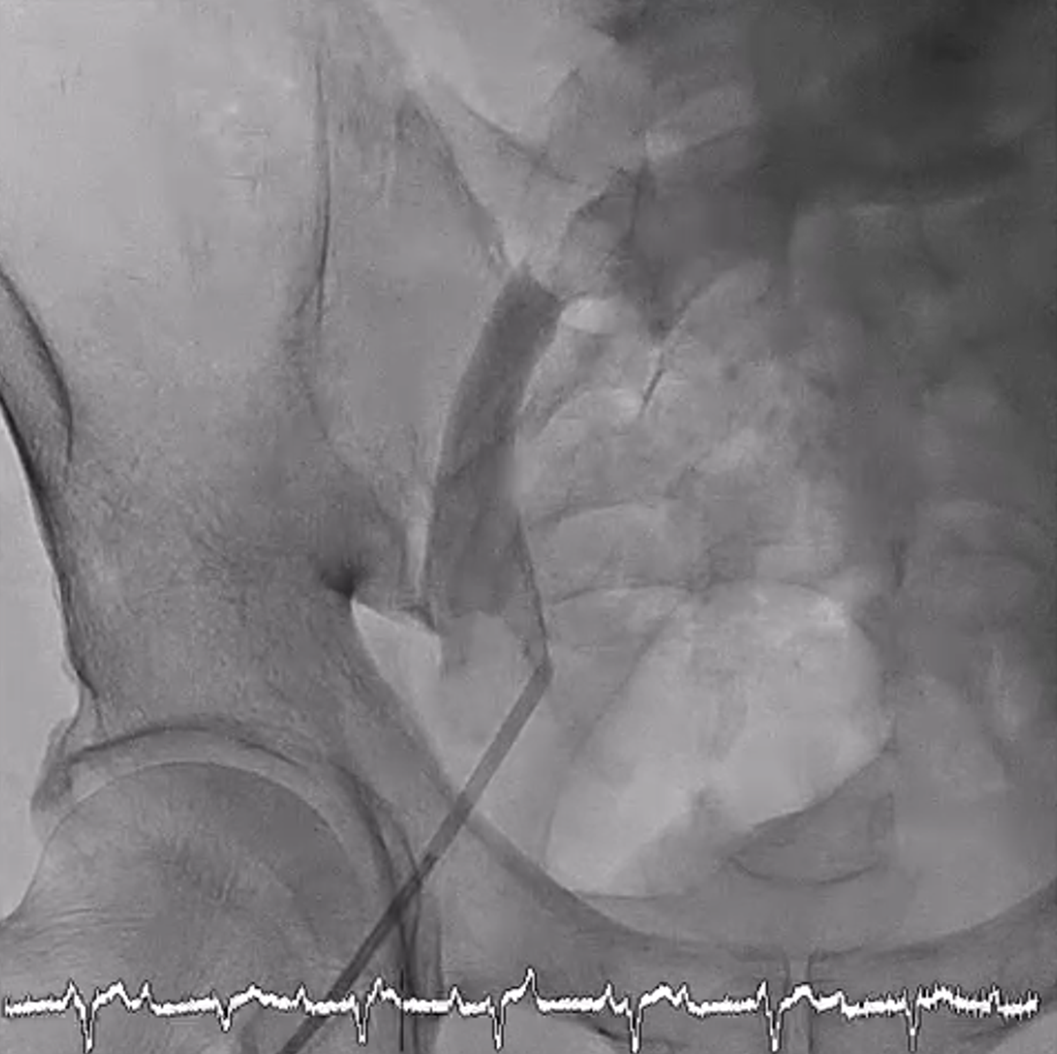
Ultrasonography-guided venous access was obtained at the right common femoral vein, and a 6F sheath was inserted. However, a 0.035-inch J-wire failed to be advanced beyond right iliac vein, with great resistance encountered. A contrast venogram was performed, which showed the appearance of a filling defect at the right common iliac vein and the venous course crossing to the left side (Figure 1, Video). Anomaly involving the lower limb veins was suspected, and the procedure was suspended.
A computed tomography (CT) venogram of the inferior vena cava (IVC) and iliac and femoral veins was arranged. The scan showed a left-sided IVC, which “crossed over” to the right side at the renal vein level (Figure 2). The apparent filling defect was attributable to external compression of the right common iliac vein by the left iliac artery as it crossed to the left side (Figure 3).



Figure 2. (A-C) Three consecutive cuts of coronal plane images (anterior to posterior) from the patient’s computed tomography venogram. The left-sided inferior vena cava is marked with an asterisk. (B) The right iliac vein appeared to be compressed by the left iliac artery (arrow), which may explain the intraprocedural finding.
Treatment options were again discussed with the patient, including a reattempt of leadless pacemaker implantation via the left common femoral vein (via a tortuous course) or reversion to a conventional transvenous pacemaker; the patient opted for the latter. The procedure was uneventful.
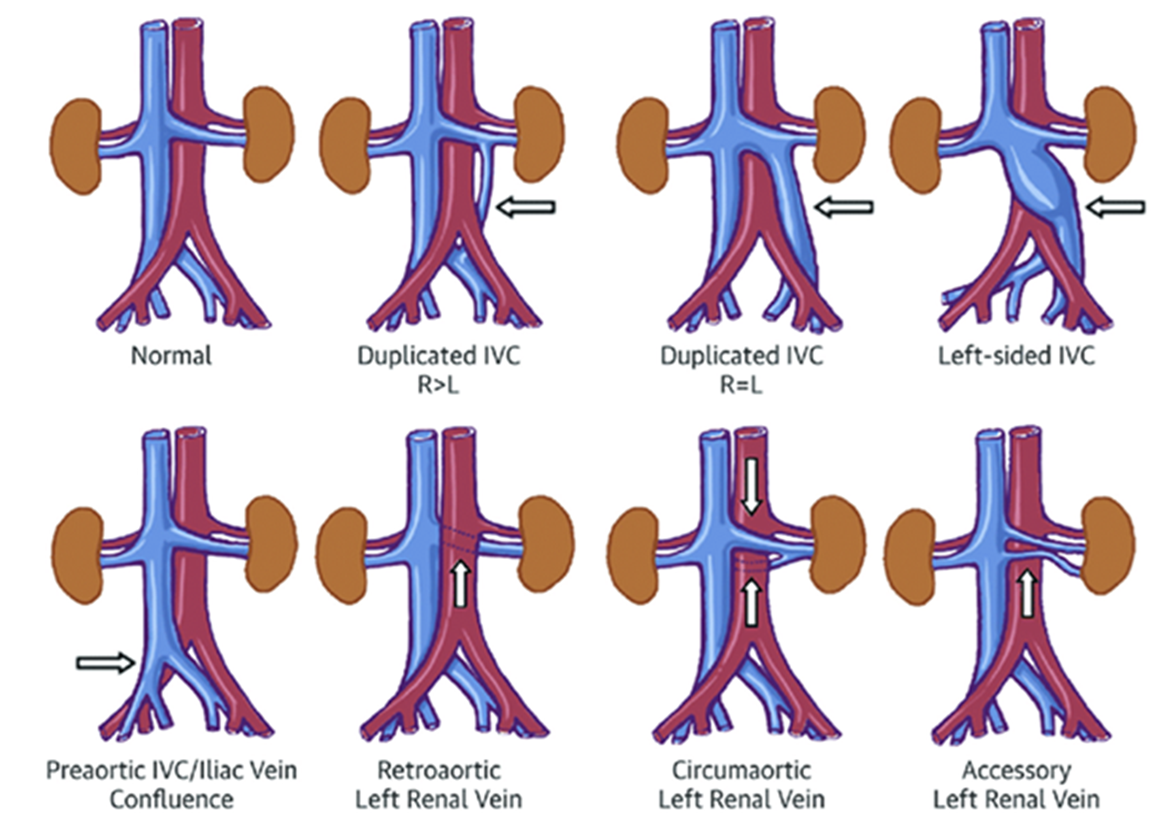
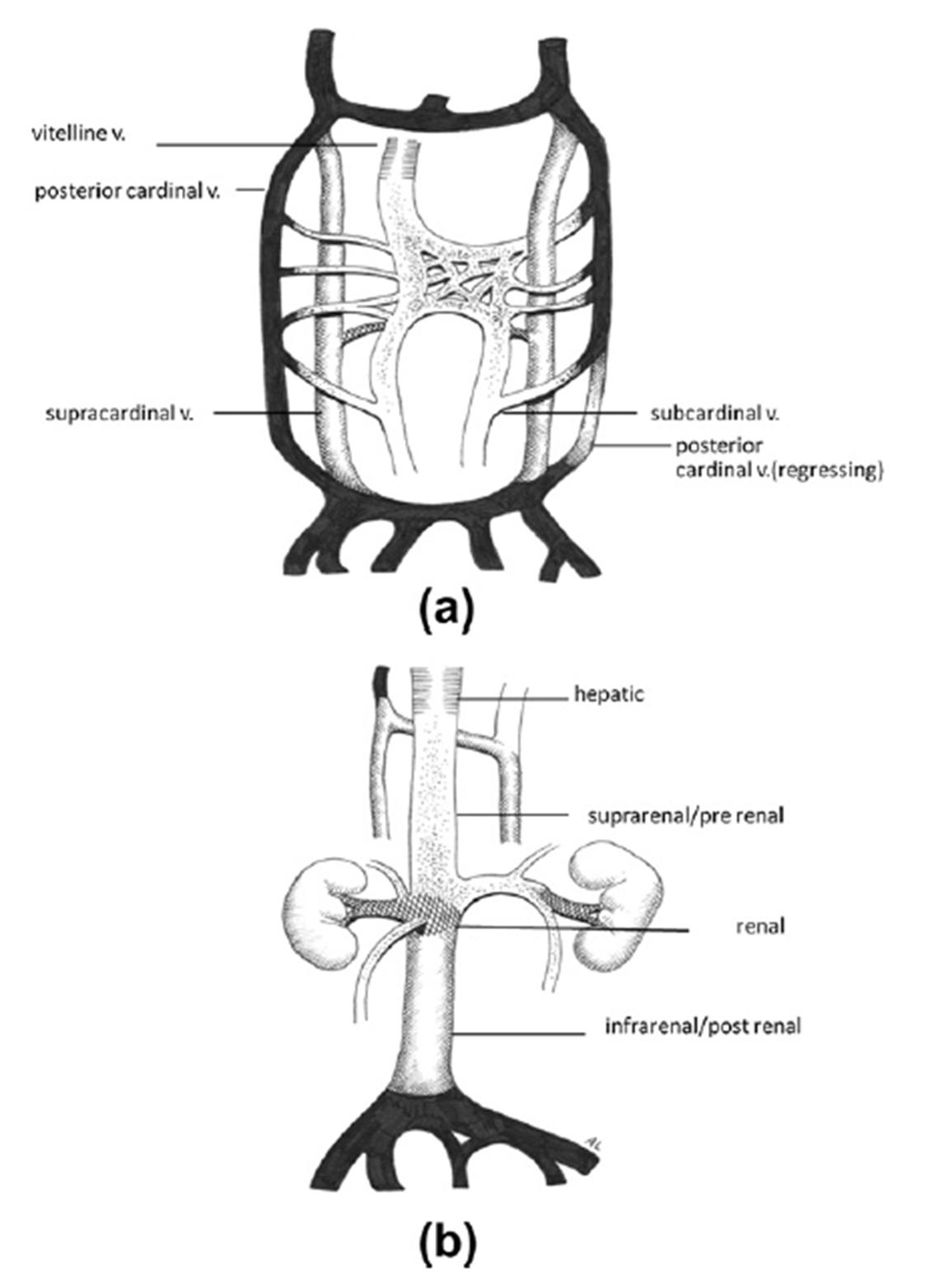
Formation of a normal IVC is a complex process. It requires anastomoses and regression (at different stages) of 3 main pairs of embryonic veins: the posterior cardinal veins, the subcardinal veins, and the supracardinal veins (Figure 4). Any errors during this process can lead to various types of IVC anomaly. For instance, left-sided vena cava is caused by the regression of the right supracardinal vein together with persistence of the left supracardinal vein.
Left-sided IVC is uncommon but clinically relevant. It brings challenges to interventional procedures involving right femoral venous access, such as leadless pacemaker implantation. Awareness of this anomaly is essential so that alternative options can be considered.
Affiliations and Disclosures
John Cheong-Hin Chan, MBBS; Kwok-Ho Yau, MBBS; Kin-Lam Tsui, MBBS, FACC
From Pamela Youde Nethersole Eastern Hospital, Chai Wan, Hong Kong.
Acknowledgments: The authors would like to thank Dr Truty and Dr Malaki for kindly allowing the use of their diagrams from their previously published work in this manuscript (Figures 3 and 4).
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the case report described in the manuscript.
Address for correspondence: John Cheong-Hin Chan, MBBS, Department of Medicine, Pamela Youde Nethersole Eastern Hospital, Lok Man Rd, Chai Wan, Hong Kong. Email: john.cheonghin.chan@gmail.com