Catch the Branch: The New Miracle Neo 3 Guidewire for Complex Bifurcation Rewiring
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
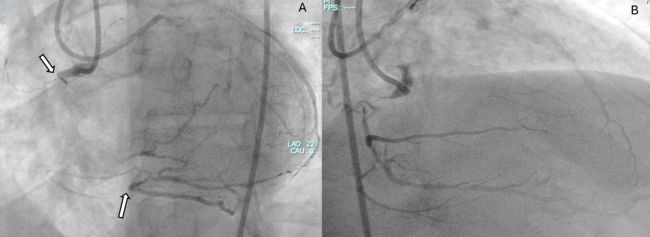
A 63-year-old man with a chronic total occlusion of the right coronary artery underwent successful recanalization using a retrograde approach. After stenting, a subocclusion of the ostial posterolateral branch occurred because of plaque shift. After several unsuccessful attempts with workhorse guidewires, the Miracle Neo 3 (MN3) (ASAHI INTECC) easily engaged the posterolateral ostium and successfully reached the distal true lumen (Figure 1; Video 1).
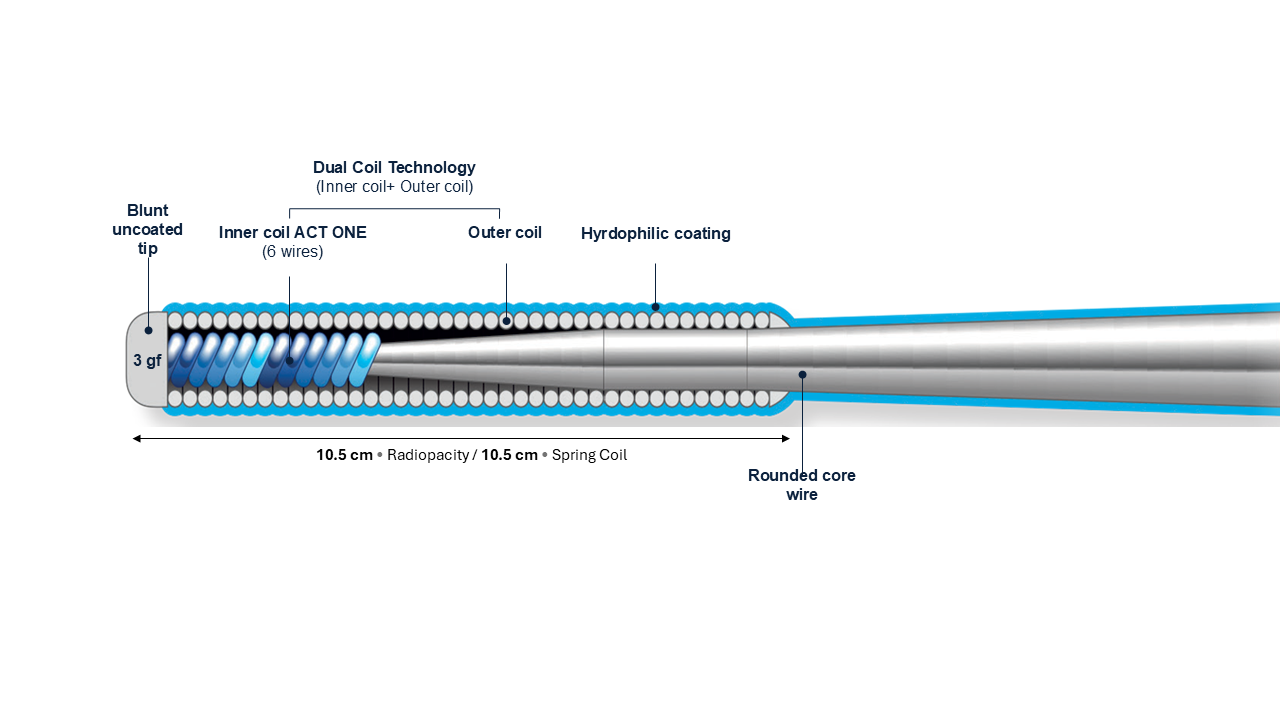
In complex bifurcation lesions, plaque/carina shift can compromise the side branch (SB) ostium, leading to prolonged attempts, failure to access the SB, or subintimal tracking, all of which are associated with increased procedural time and complication risk. An ideal guidewire for difficult SB rewiring should have a low penetration force to maximize safety, enhanced torque control for precise steering, excellent trackability for smooth advancement, and moderate tip stiffness to prevent prolapse during manipulation. The MN3 guidewire embodies these features (Figure 2), making it well suited for difficult SB rewiring. Despite a tip load of 3 g, the MN3 maintains a safety profile because of its tip design, resulting in low penetration force. The penetration force depends on the ratio between the tip load and surface area; the blunt-tip design increases surface area, reducing the penetration force to about 24 gf/mm², only slightly higher than workhorse guidewires (10-21 gf/mm²).
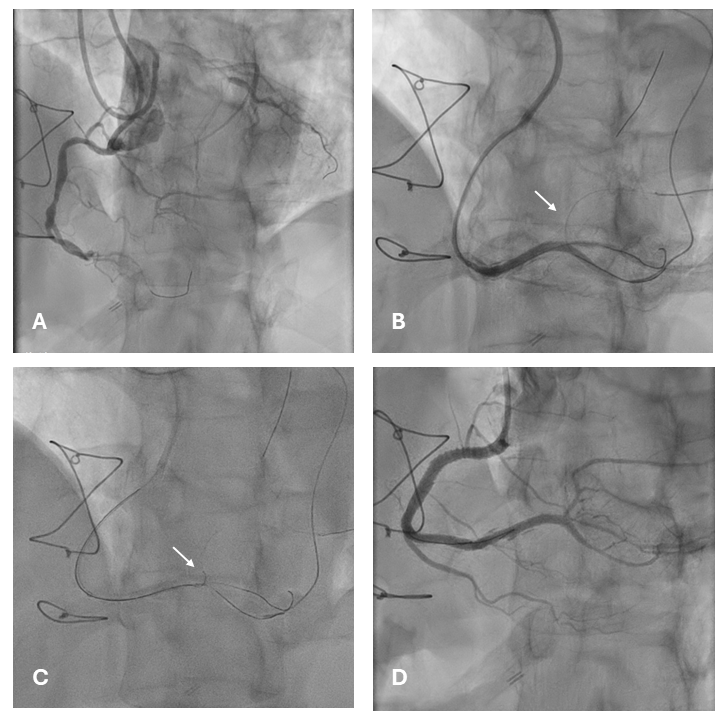
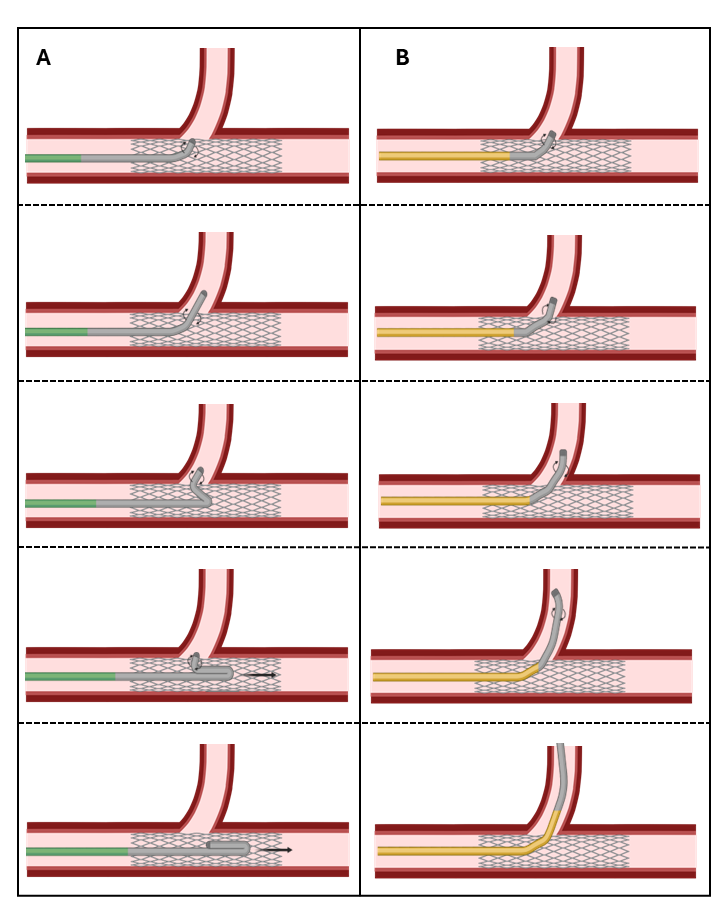
Another key feature is its stiffness. Guidewire stiffness, influenced by tip load and coiled segment length, affects resistance to bending. The MN3, having a moderately weighted tip and a short-coiled segment (10.5 cm), is stiffer than workhorse guidewires. During SB rewiring, highly flexible workhorse guidewires tend to prolapse once the SB ostium is engaged, whereas the moderate stiffness of the MN3 provides better shaft support, reducing prolapse (Figure 3, Video 2). Importantly, the low penetration force enhances safety not only during crossing but also during device delivery, obviating the need for guidewire exchange after successful rewiring.
Affiliations and Disclosures
Gabriele L. Gasparini, MD1; Laura Novelli, MD1,2; Jacopo A. Oreglia, MD3; Yoshihisa Kinoshita, MD4; Jorge Sanz-Sanchez, MD, PhD5,6
Dr Gasparini and Dr Novelli contributed equally to this manuscript.
From the 1IRCCS Humanitas Research Hospital, Rozzano-Milan, Italy; 2Department of Biomedical Sciences, Humanitas University, Pieve Emanuele-Milan, Italy; 3Interventional Cardiology, De Gasperis Cardio Center, Niguarda Hospital, Milan, Italy; 4Division of Cardiovascular Medicine, Toyohashi Heart Center, Aichi, Japan; 5Centro de Investigación Biomedica en Red (CIBERCV) – Madrid, Spain; 6Hospital Universitari i Politecnic La Fe, Valencia, Spain.
Acknowledgments: The authors thank ASAHI INTECC for the use of the Educational Total Occlusion Simulation System (ETOSS) simulator.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and for the publication thereof, including any and all images
Address for correspondence: Gabriele L. Gasparini, MD, Department of Biomedical Sciences, Humanitas University, Via Rita Levi Montalcini 4, 20090 Pieve Emanuele, Milan, Italy. Email: gabriele._luigi.gasparini@humanitas.it