

Ventricularization of Right Atrial Pressure
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
A 76-year-old man with hypothyroidism, chronic obstructive pulmonary disease, and coronary artery disease presented with dyspnea (New York Heart Association Class III), facial puffiness, and bilateral pitting pedal edema for the past 3 months. He had undergone percutaneous coronary intervention to the right coronary artery (RCA) and obtuse marginal major artery (OMM) in 2017 and the first diagonal in 2021. At presentation, his jugular venous pressure was raised with giant C-V waves. The 12-lead electrocardiogram showed sinus rhythm, right bundle branch block, and intermittent multifocal atrial premature complexes. Two-dimensional echocardiography revealed torrential-free tricuspid regurgitation (TR), moderate pulmonary artery hypertension, and moderate right ventricle (RV) dysfunction with near-normal left ventricle function.
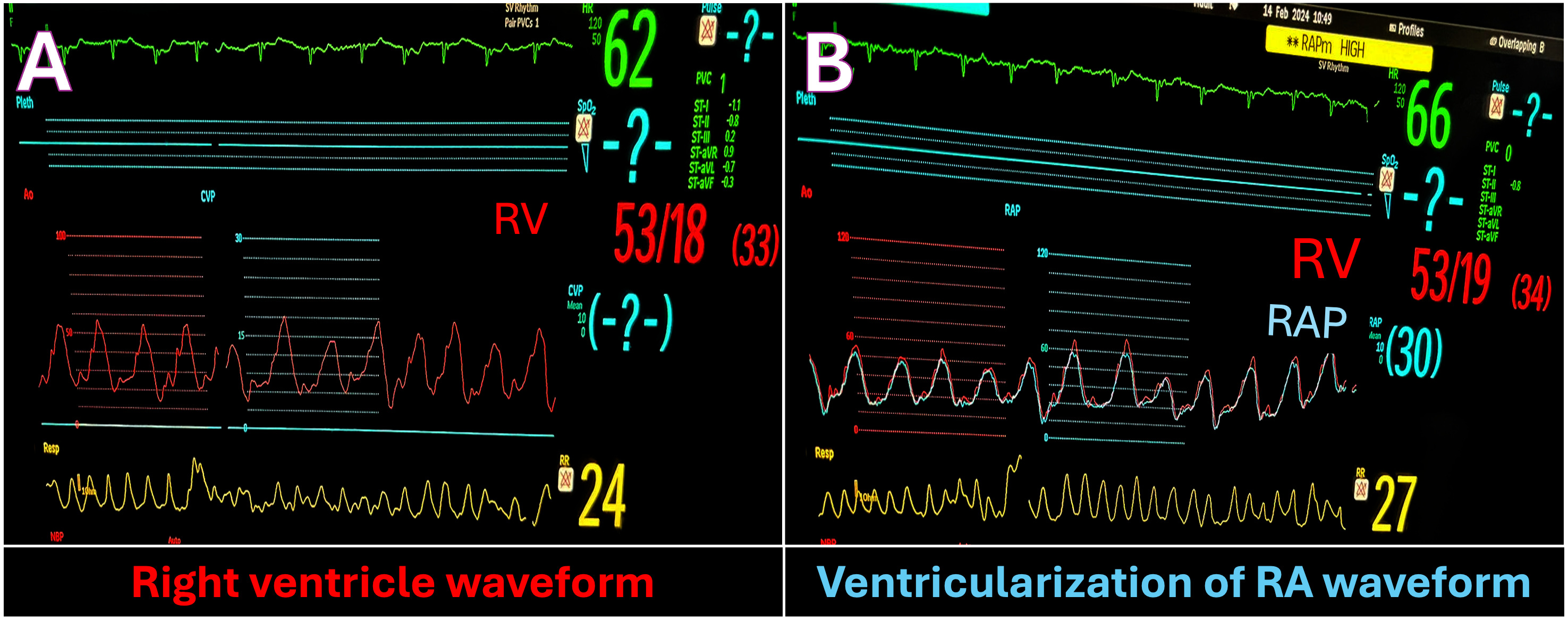
The patient was taken up for a coronary angiography with right heart catheterization. There was significant disease in the mid-left anterior descending artery and mild in-stent restenosis in the OMM and patent RCA stents. The catheterization study revealed a high RV end-diastolic pressure (EDP) of 18 mm Hg (normal: 1-7 mm Hg) and elevated right atrial (RA) pressures (mean RA pressure: 30 mm Hg) (Figure). The RA pressure trace had large V waves (53 mm Hg), and the prominent Y descent and RA trace resembled RV trace, characteristically known as ventriculization of RA pressure. The RV angiogram revealed grade 4 TR (Video). There was moderate pulmonary arterial hypertension (PA systolic pressure: 49 mm Hg; diastolic pressure: 27 mm Hg; and mean PA pressure: 38 mm Hg) and the left ventricle EDP was 9 mm Hg. The final diagnosis was right heart failure secondary to type 3 pulmonary hypertension. The patient was planned for medical management and doing well on diuretics.
Ventricularization of the RA pressure trace is a very rare phenomenon in severe free TR. The RA trace resembles the RV trace except that it is of lower amplitude. Some differential diagnoses include atrial septal defect with gross heart failure, and burnt-out RV diseases such as endomyocardial fibrosis.
Affiliations and Disclosures
Neha Chopra, MD, DM1; Shitij Chaudhary, MD2; Sourabh Agstam, MD, DM2; Sivasubramanian Ramakrishnan, MD2
From the 1Department of Cardiology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India; 2Department of Cardiology, All India Institute of Medical Sciences, New Delhi, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and for the publication, including photographs.
Address for correspondence: Sourabh Agstam, MD, DM, Department of Cardiology, 7th Floor, Cardio-Thoracic Centre, All India Institute of Medical Sciences, New Delhi 110029, India. Email: sourabhagstam@gmail.com; X: @agstamsourabh










