

UNICORN With Self-Expanding Valves: A Recrossing Technique to Achieve Stepwise Leaflet Opening and Seamless Valve Deployment
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
With balloon-expandable valves, the UNICORN technique enables simultaneous leaflet laceration and valve deployment through a purposedly created leaflet fenestration.1,2 However, similar intra-leaflet deployment was not previously feasible with self-expanding valves (SEV).3,4 In the following steps, we describe a novel recrossing technique that facilitates near-simultaneous leaflet laceration and SEV deployment (Video).
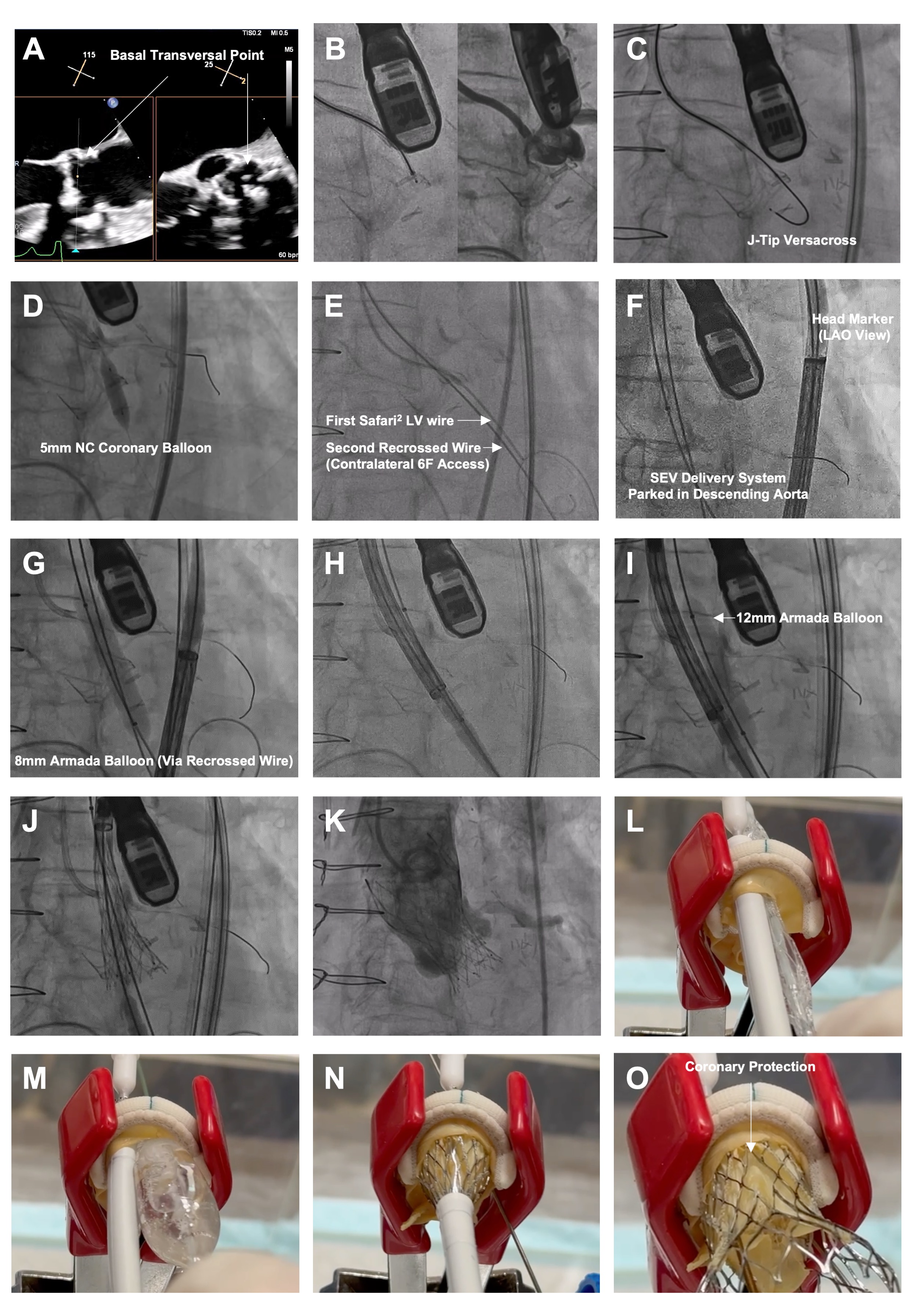
- Position a 7F guide (left: Amplatz Left 1/2; right: Multipurpose), 135-cm NaviCross catheter (Terumo), and 0.035-inch J-tip VersaCross wire (Boston Scientific) at the base of the target leaflet (Figure A and B). Traverse with radiofrequency (Figure C), cross the microcatheter, and exchange for a 300-cm coronary guidewire.
- Dilate fenestration with a 5-mm noncompliant coronary balloon (Figure D). Cross the microcatheter and exchange for a pre-shaped stiff wire. Recross the fenestration from contralateral 6F access with a second guidewire (0.035-inch straight-tip EMERALD [Cordis] or J-tip [Terumo]), using a similar 7F guide (Figure E). Exchange the second wire for an Amplatz Extra Stiff (Cook Medical).
- Deliver an Evolut FX+ valve (Medtronic) via primary access to the descending aorta, with the head marker oriented along the outer curvature under left anterior oblique projection to facilitate commissural alignment (Figure F).
- Dilate the fenestration with an 8-mm peripheral balloon via contralateral access (Figure G); this facilitates subsequent crossing of the SEV. The target leaflet is not lacerated at this stage.
- Position a 12-mm peripheral balloon and the SEV delivery capsule side by side across the fenestration. (Figure H). Gradually inflate the balloon until “give-way,” indicating leaflet laceration (Figure I). Deploy the SEV (Figure J) and simultaneously deflated balloon, and withdraw the guidewire. Controlled pacing may enhance stability. Near-simultaneous leaflet laceration and SEV deployment preserves hemodynamics; it also entraps the lacerated leaflet and places it away from the coronary ostium if the balloon pushes the SEV toward the annulus. (Figure-1K/1L)
- If the leaflet is lacerated during the second balloon dilatation, withdraw the balloon and advance the SEV from the aorta for seamless deployment.
In conclusion, the UNICORN with recrossing technique enables seamless leaflet laceration and SEV deployment (Figure M-O).
Affiliations and Disclosures
Simon Cheung-Chi Lam, MBBS1,2; Kwong-Yue Eric Chan, MBBS1,2,3; Shu-Yue Sze, MBBS1,2; Daniel Tai-Leung Chan, MBBS4,5; Ho-On Alston Conrad Chiu, MBBS1,2; Ka-Chun Un, MBBS MRes(Med)1,2; Frankie Chor-Cheung Tam, MBBS1,2; Gilbert H.L. Tang, MD, MSc, MBA6; Chun-Ka Wong, MBBS1,2
From the 1Cardiology Division, Department of Medicine, School of Clinical Medicine, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Hong Kong SAR, China; 2Cardiology Division, Department of Medicine, Queen Mary Hospital, Hong Kong SAR, China; 3Cardiac Medical Unit, Grantham Hospital, Hong Kong SAR, China; 4Department of Cardiothoracic Surgery, Queen Mary Hospital, Hong Kong SAR, China; 5Department of Surgery, School of Clinical Medicine, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Hong Kong SAR, China; 6Department of Cardiovascular Surgery, Mount Sinai Health System, New York.
Mr Lam, Mr K-Y E Chan, Mr Sze, Mr D T-L Chan, Mr Chiu, and Mr Un contributed equally to this work.
Disclosures: Dr Tang has received speaker honoraria from, and has served as a physician proctor, consultant, advisory board member, TAVR publications committee member, APOLLO trial screening committee member, and IMPACT MR steering committee member for Medtronic; has received speaker honoraria from, and has served as a physician proctor, consultant, advisory board member, and TRILUMINATE trial anatomic eligibility and publications committee member for Abbott Structural Heart; has served as an advisory board member for Boston Scientific and JenaValve; has served as a consultant and physician screening committee member for Shockwave Medical; has served as a consultant for NeoChord, Peija Medical, and Shenqi Medical Technology; and has received speaker honoraria from Siemens Healthineers. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Chun-Ka Wong, MBBS, Department of Medicine, The University of Hong Kong, Hong Kong SAR, China. Email: wongeck@hku.hk
References
1. Chan KE, Chan DT, Lam CS, et al. First-in-human undermining iatrogenic coronary obstruction with radiofrequency needle (UNICORN) procedure during valve-in-valve transcatheter aortic valve replacement. Circ Cardiovasc Interv. 2022;15(11):928-931. doi:10.1161/CIRCINTERVENTIONS.122.012399
2. Chan KE, Wong CK, Chan TL, Tang GHL, Lam SC. Letter to the editor: recommended steps for UNICORN with balloon-expandable valves. JACC Cardiovasc Interv. 2025:S1936-8798(25)01629-2. doi:10.1016/j.jcin.2025.05.034
3. Haberman D, Lupu L, Merdler I, et al. UNICORN with a self-expanding valve to treat a degenerated balloon-expandable valve. JACC Cardiovasc Interv. 2025;18(1):123-125. doi:10.1016/j.jcin.2024.09.048
4. Mew C, Dahiya A, Chong AA, et al. First-in-human: leaflet laceration with balloon mediated annihilation to prevent coronary obstruction with radiofrequency needle (LLAMACORN) for valve-in-valve transcatheter aortic valve replacement. Catheter Cardiovasc Interv. 2024;104(5):1079-1085. doi:10.1002/ccd.31195










