

Scimitar Syndrome
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
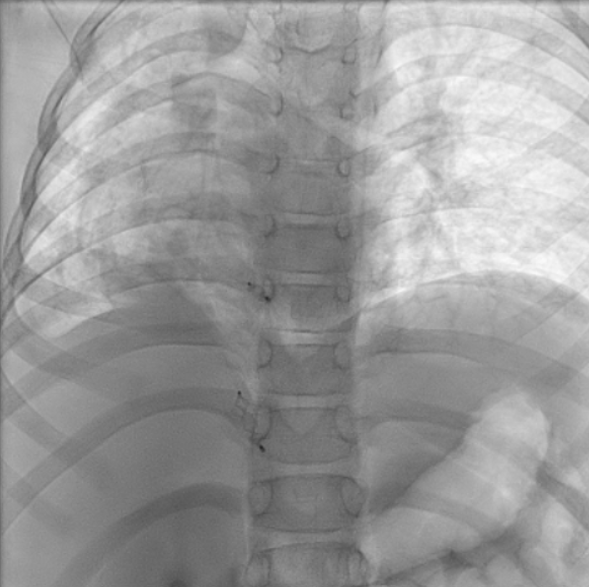
An 8-year-old girl presented with persistent pneumonia of a 1-month duration and right lower zone opacity on chest x-ray. Computed tomography of her thorax revealed right lung hypoplasia with partial anomalous pulmonary venous drainage (PAPVD) of the right pulmonary veins into the inferior vena cava. Two prominent aortopulmonary collaterals (APCs) supplying the right lung were noted—one from the descending thoracic aorta (DTA) and one from the celiac artery—along with 2 minor APCs from the DTA (Figure 1). These features were consistent with Scimitar syndrome, named after its visual resemblance to the Turkish sword (Video 1, Figure 2).
Following resolution of pneumonia, the child underwent cardiac catheterization, which confirmed dual arterial supply to the right lung via the right pulmonary artery and APCs. It was decided to redirect flow and reduce shunting using vascular plugs. First, femoral access was obtained with a 5F catheter. Next, a digital subtraction aortogram was performed with a 5F pigtail catheter. The prominent APC from the DTA measured 3.1 mm; it was hooked with a 5F Judkins right (JR) guiding catheter. A 4 x 6-mm Amplatzer Vascular Plug II (Abbott) was then deployed into the APC under angiographic guidance. The APC from the celiac artery measured 3.2 mm; it was hooked with a 5F JR guiding catheter. A 6 x 6-mm Amplatzer Vascular Plug II was deployed into the APC under angiographic guidance. The prominent APCs were successfully occluded (Figure 3), and post-deployment angiogram showed good position and good flows in the celiac artery and its other branches (Video 2).
This case highlights the characteristic features of Scimitar syndrome, including PAPVD and anomalous systemic arterial supply, managed effectively with targeted intervention.


Affiliations and Disclosures
Gayathri Bhuvaneswaran Kartha, DM; Shruti Irene Varghese, DM; Anoop George Alex, DM; Oommen K. George, DM
From the Department of Cardiology, Christian Medical College, Vellore, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the parents for publication of their child's data, including any and all images.
Address for correspondence: Gayathri Bhuvaneswaran Kartha, DM, Department of Cardiology, Christian Medical College, Vellore, India. Email: gbksignsin@gmail.com










