

Plaque Modification Using the New LithiX Hertz Contact Intravascular Lithotripsy Balloon and a Super High-Pressure OPN NC Balloon in a Severely Calcified Coronary Artery With Undilatable Plaque: A Case Report
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
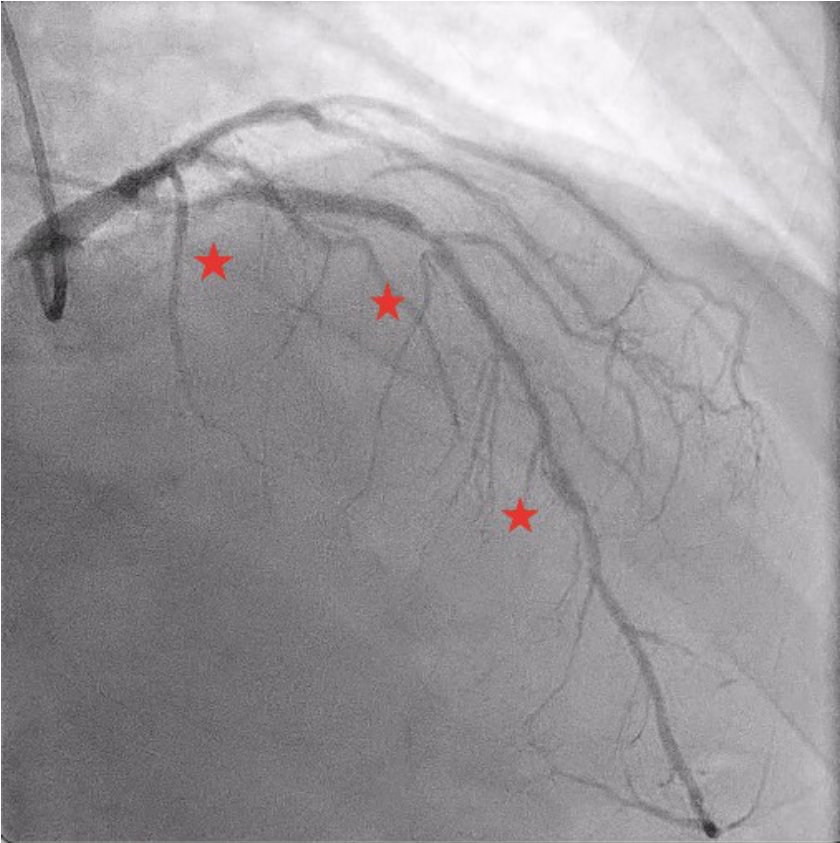
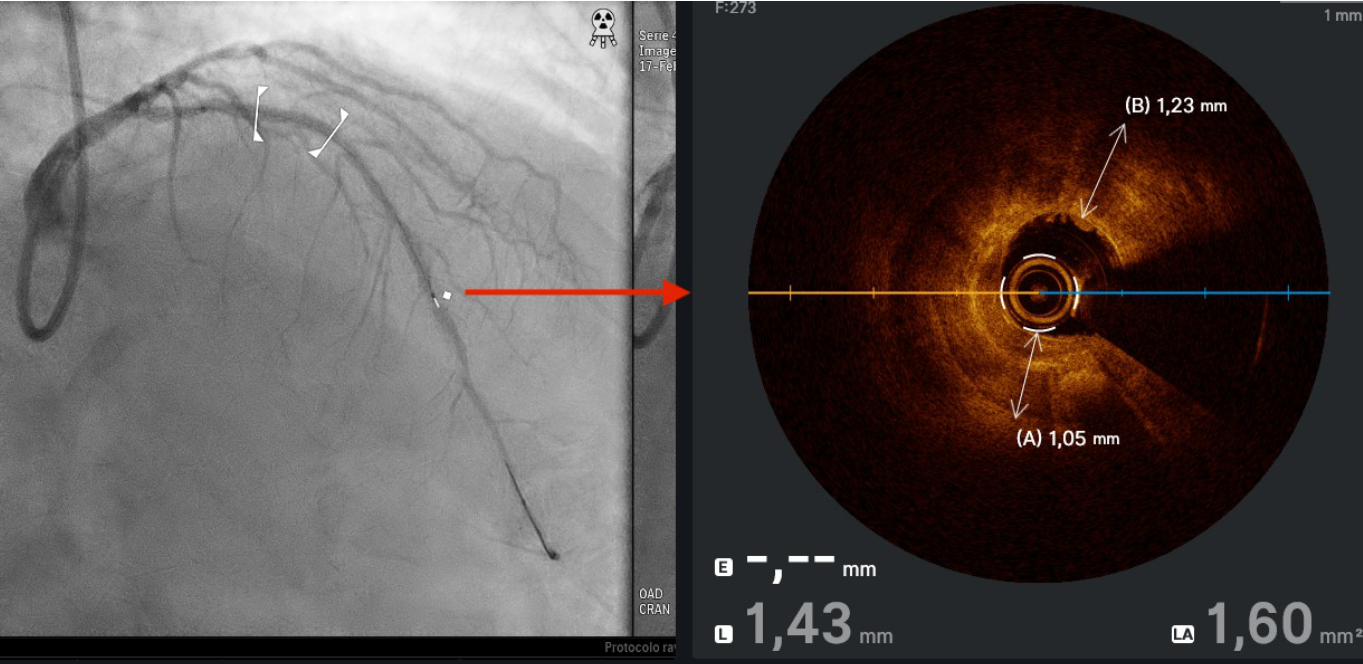
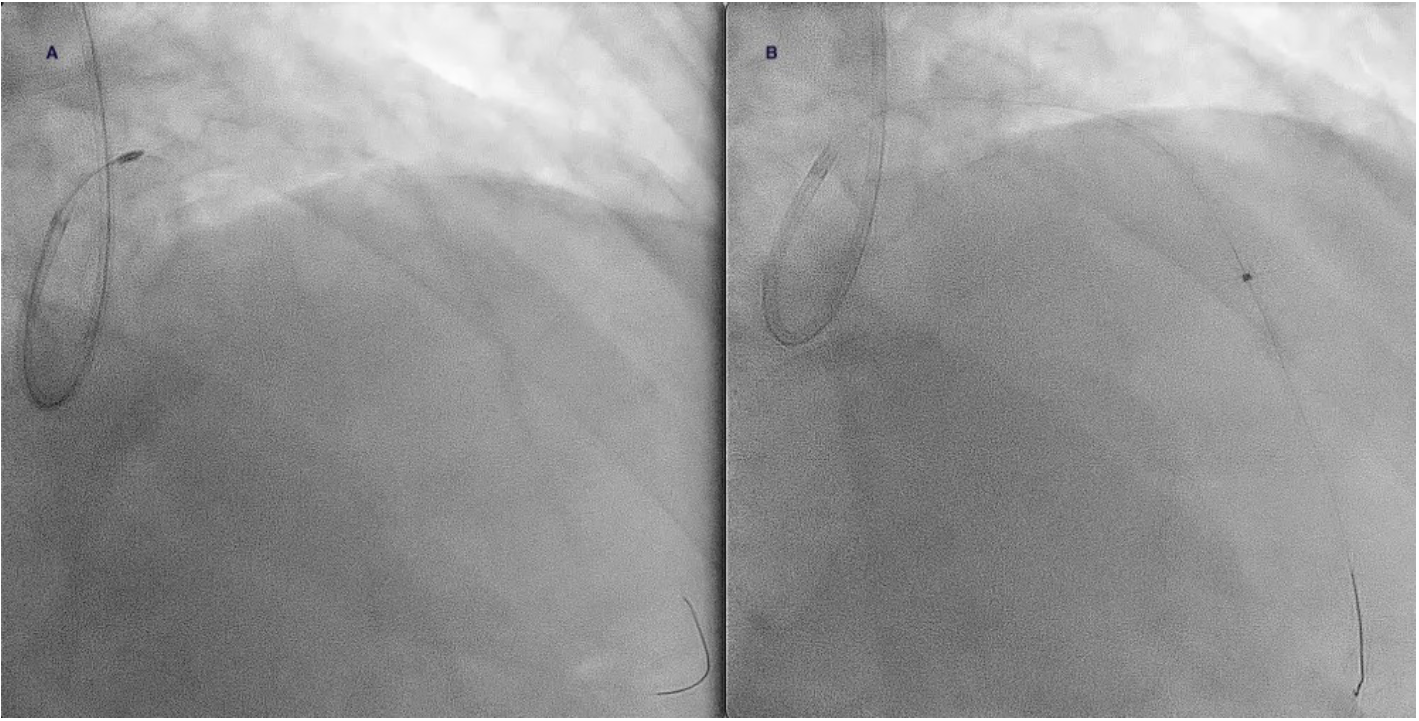
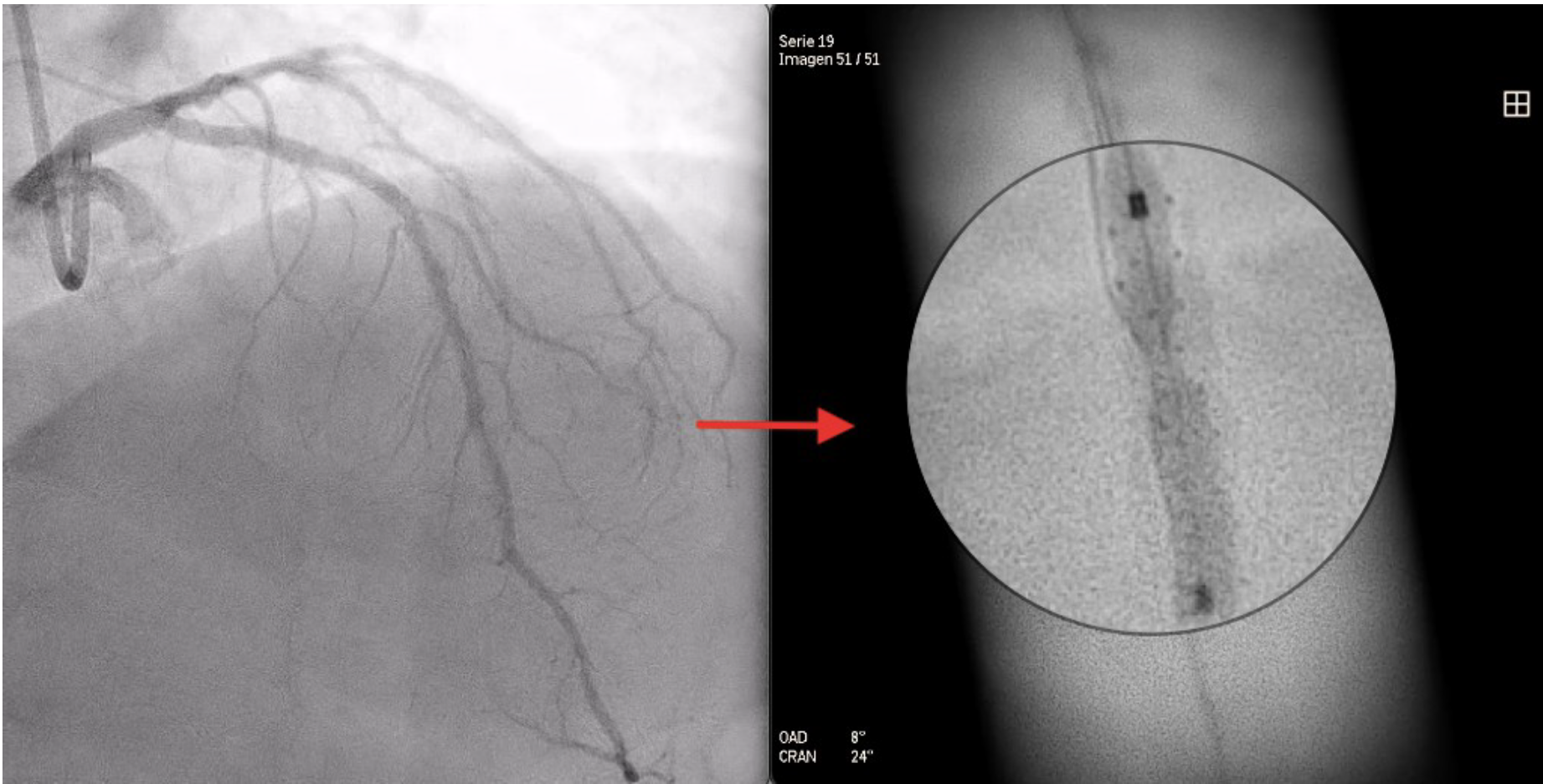
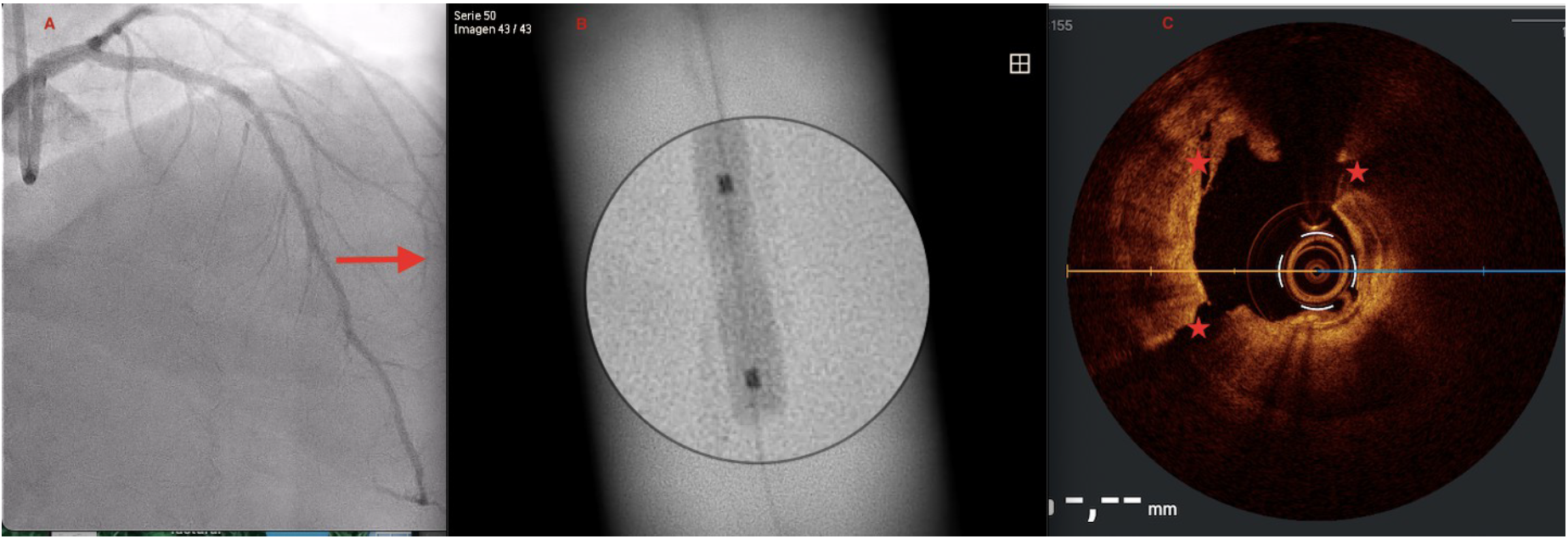
A 73-year-old man was hospitalized with acute coronary syndrome. Angiography showed severely calcified disease in the anterior descending artery and severe stenosis in the proximal, medial, and distal segments (Figure 1). Angioplasty was performed with an NC Trek Neo balloon (Abbott) with proper preparation of the plaque in the proximal and medial segments. Optical coherence tomography showed calcified plaque with a 360° ring and 1.2-mm thickness in the distal segment (Figure 2). Expansion attempts using a super high-pressure 2.5 x 10-mm OPN NC percutaneous transluminal coronary angioplasty (PTCA) balloon (SIS Medical) failed to fracture the calcification; rotational atherectomy with a Rotablator (Boston Scientific) was also unsuccessful. A 1.4-mm excimer laser coronary atherectomy catheter (Spectranetics) was also used (Figure 3) without fracturing the calcification, even after attempts with a super high-pressure balloon at 45 to 50 atm and being inflated for 40 to 60 seconds (Figure 4). Finally, a 3 x 28-mm Angiolite sirolimus-eluting stent (iVascular) was deployed in the proximal segments, followed by a 2.5 x 35-mm paclitaxel-eluting balloon (Medtronic) in the medial segment.
The distal lesion was treated in a deferred session using the LithiX Hertz Contact intravascular lithotripsy system (HC-IVL) (Elixir Medical) (Figure 5), which features a new intravascular catheter with mechanical contact indicated for fragmentation of newly appearing calcified, stenotic lesions in a coronary artery with moderate to serious calcifications before stent insertion. The LithiX HC-IVL’s unique design incorporates stainless steel hemispheres into a semi-compliant balloon; these hemispheres create different pressure points that help fracture calcified plaque via mechanical contact force.
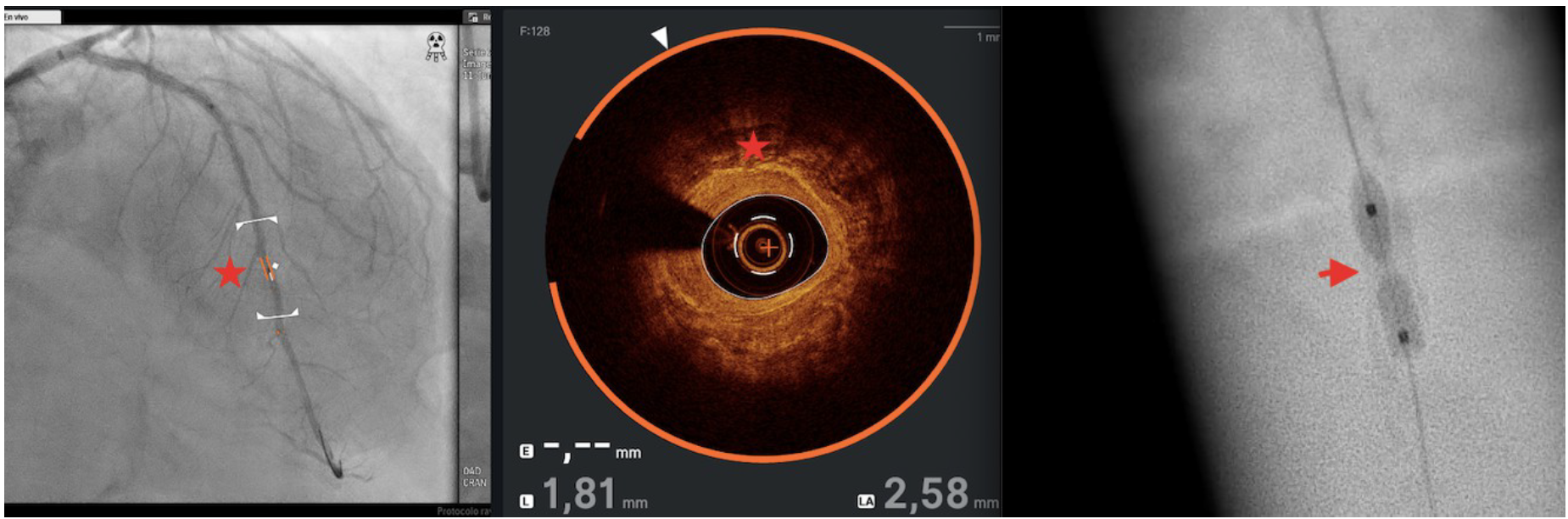
After progressive dilations, maintaining pressures from 8 to 20 atm with a LithiX HC-IVL 2.5 x 10-mm balloon, dilation was performed with a 2.5 x 10-mm OPN NC PTCA balloon at 35 atm for 30 seconds and fracture of the calcium ring was achieved (Figure 6). The patient was discharged without complications or events during follow-up.
This plaque modification strategy combines new technology with the LithiX HC-IVL balloon and a super high-pressure OPN NC balloon after a failed attempt with rotational atherectomy and a coronary laser with a super high-pressure balloon. The experience suggests that the combined use of the LithiX HC-IVL balloon and a super-high pressure balloon can be effective in undilatable lesions with a high degree of calcification.
Affiliations and Disclosures
Oscar Lagos Degrande, MD; Carmen Lluch Requerey, MD; Miguel Angel Montilla, MD; Santiago Camacho Freire, PhD; Jessica Roa Garrido, MD; Elena Izaga, PhD; Antonio Gomez Menchero, MD
From the Juan Ramón Jiménez University Hospital: Hospital Universitario Juan Ramon Jimenez, Huelva, Spain.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient(s) for the intervention(s) described in the manuscript and for the publication thereof, including any and all images.
Address for correspondence: Oscar Lagos Degrande, MD, Calle Opera Carmen 42, 41007, Seville, Spain. Email: oldeg2450@gmail.com; X: @DegrandesLagosDr










