

Percutaneous Mechanical Aspiration Prior to Transvenous Lead Extraction and Implantable Cardioverter Defibrillator Removal in Infective Endocarditis
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Cardiovascular implantable electronic device (CIED) infective endocarditis with large vegetations requires transvenous extraction.1 However, vegetations greater than 2 cm in length have a high embolization risk and require surgical removal.1,2
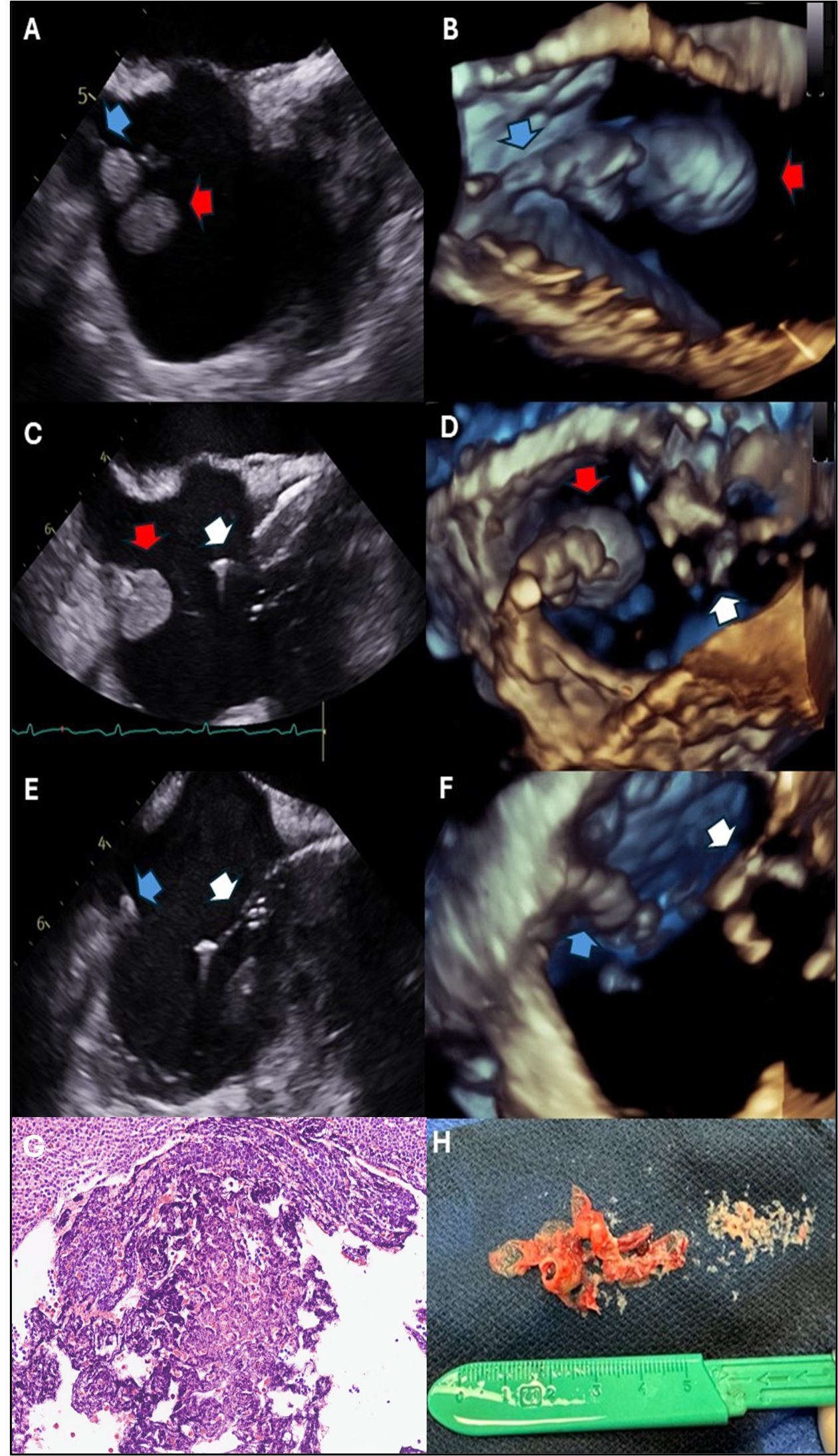
A 59-year-old man with heart failure with reduced ejection fraction (HFrEF) and a single-chamber implantable cardioverter-defibrillator presented with group B streptococcus bacteremia. Transesophageal echocardiography (TEE) revealed a 2.4 x 1.5-cm vegetation on the atrial portion of the right ventricular lead (Figure A and B). Due to the embolization risk with extraction alone, percutaneous mechanical aspiration (PMA) using the AngioVac system (AngioDynamics) was pursued. The AngioVac system, consisting of aspiration cannulas connected to a veno-venous perfusion circuit, was inserted via the right internal jugular vein. Under TEE guidance, the aspiration catheter removed the vegetation (Figure C-F) and then repositioned to capture residual vegetative material. The lead was successfully extracted and pathology confirmed infection (Figure G and H). For CIED vegetations, percutaneous mechanical aspiration followed by extraction may reduce embolization risk.
Affiliations and Disclosures
Faaiq N. Aslam, MD1; Kevin Tayon, MD2 ; Jeanwoo Yoo, DO2 ; Abdallah El Sabbagh, MD2; Danesh Kella, MBBS2 ; Christoffel J. van Niekerk, MD2
From the Departments of 1Internal Medicine and 2Cardiovascular Diseases, Mayo Clinic, Jacksonville, Florida.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient(s) for the intervention(s) described in the manuscript and for the publication othereof, including any and all images.
Address for correspondence: Christoffel J. van Niekerk, MD, Mayo Clinic Department of Cardiovascular Disease, 4500 San Pablo Road, Jacksonville, FL 32224, USA. Email: vanniekerk.christoffel@mayo.edu
References
1. Kusumoto FM, Schoenfeld MH, Wilkoff BL, et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm. 2017;14(12):e503-e551. doi:10.1016/j.hrthm.2017.09.001
2. Arora Y, Perez AA, Carrillo RG. Influence of vegetation shape on outcomes in transvenous lead extractions: does shape matter? Heart Rhythm. 2020;17(4):646-653. doi:10.1016/j.hrthm.2019.11.015










