

Orbital Atherectomy for Calcified Nodules Following Insufficient Deformation by Intravascular Lithotripsy
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
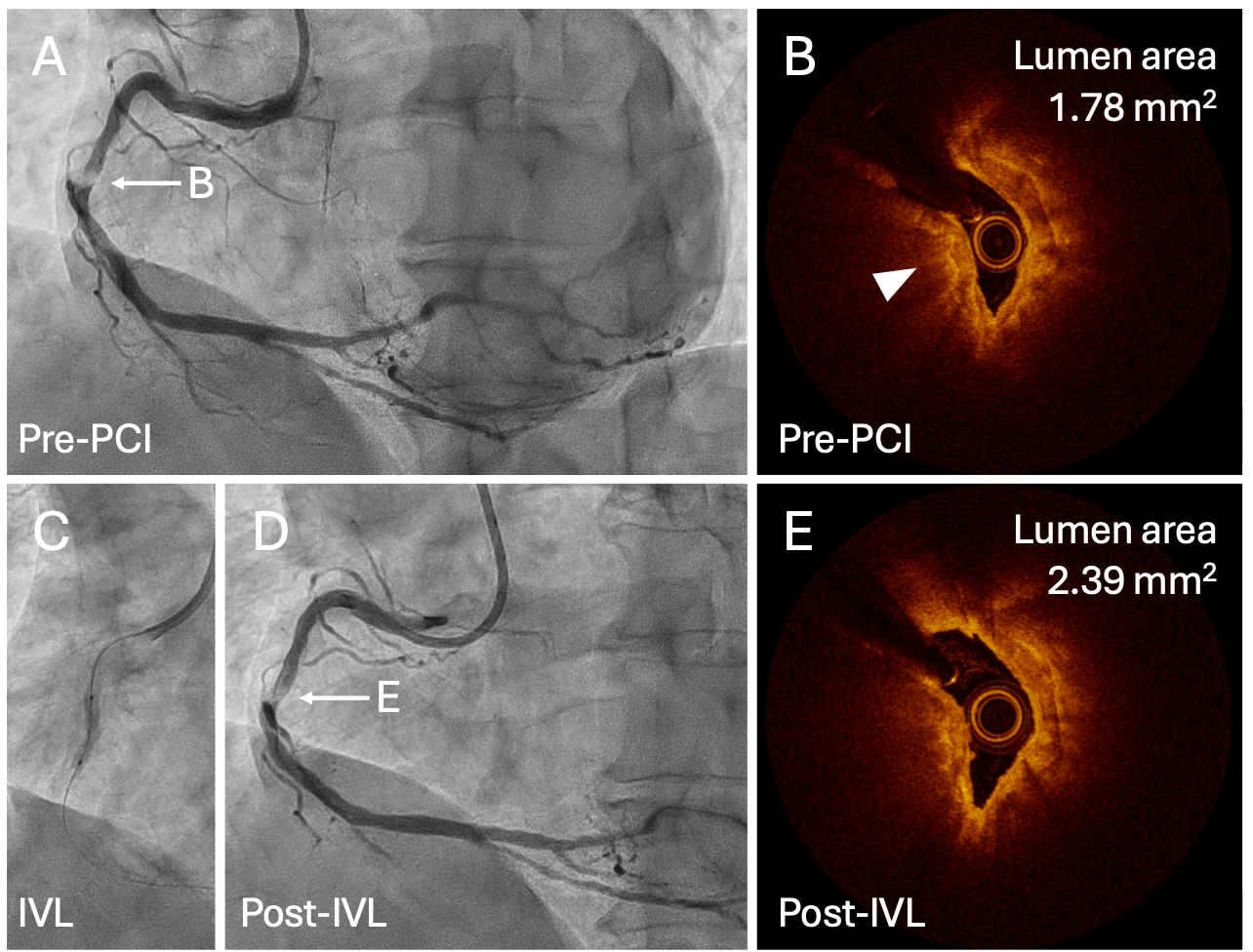
A 60-year-old man with diabetes mellitus presented to the hospital with chronic coronary syndrome. Coronary angiography (CAG) revealed a severely calcified lesion in the proximal right coronary artery (RCA) (Figure A). After low-profile balloon dilatation, optical coherence tomography (OCT) showed calcified nodules (CNs) in the proximal RCA (Figure B) and the proximal reference lumen diameter was 3.5 mm.
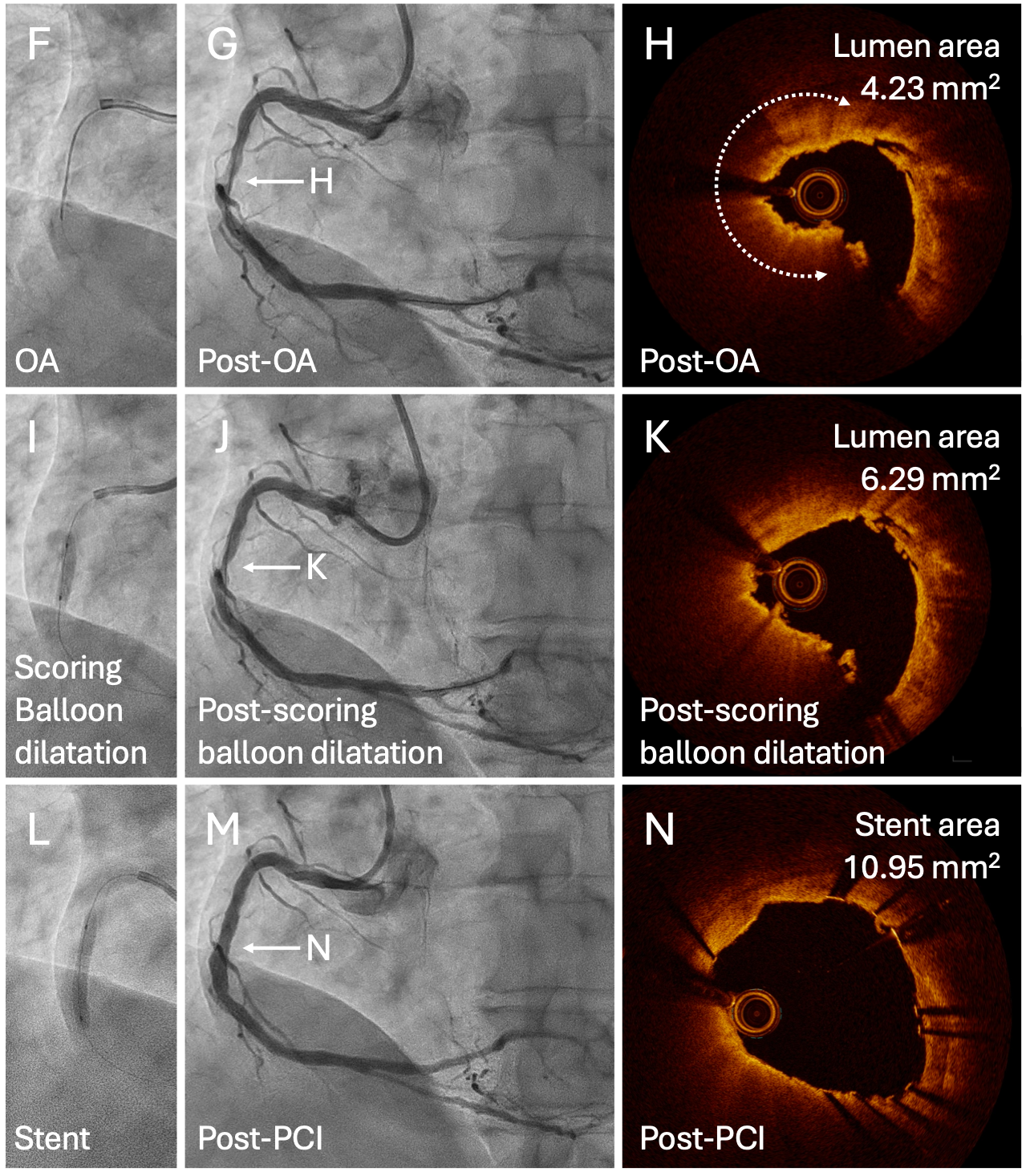
It was decided to use a 3.5-mm intravascular lithotripsy (IVL) balloon (Shockwave C2; Shockwave Medical, Inc.) to modify the calcified components (Figure C). However, even after 80 pulses, the IVL balloon expansion was insufficient (Figure D and E). Since further lumen gain was unlikely to be achieved with modified balloon dilatation, orbital atherectomy (OA) was performed with the Diamondback 360 system (Abbott) at low- and high-speed rotations (Figure F).
Post-OA OCT revealed significant debulking of calcium at the CN site (Figure G and H). The lesion was predilated with a 3.5-mm scoring balloon, and acceptable lumen enlargement was obtained (Figure I-K). Subsequently, a 3.5 × 23 mm drug-eluting stent was deployed and postdilated with a 4.5-mm noncompliant balloon because the vessel diameter in the mid-portion of the lesion was 4.5 mm on OCT imaging. (Figure L). The final CAG and OCT images showed acceptable stent expansion (Figures M and N), and no cardiovascular events occurred 3 months after the procedure.
The management of heavily calcified lesions with CNs remains challenging.1 Although the efficacy of IVL for CNs has been previously reported, approximately one-fourth of CNs are not deformable after IVL.2 To the best of our knowledge, this is the first case report demonstrating successful OA modification of CNs after insufficient IVL treatment.
Affiliations and Disclosures
Toru Misawa, MD, PhD1; Tetsumin Lee, MD, PhD1; Takashi Ashikaga, MD, PhD1; Toshihiro Nozato, MD PhD1; Taishi Yonetsu, MD, PhD2; Tetsuo Sasano, MD, PhD2
From the 1Department of Cardiology, Japanese Red Cross Musashino Hospital, Tokyo, Japan; 2Department of Cardiovascular Medicine, Institute of Science Tokyo, Tokyo, Japan.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and for the publication of his data.
Address for correspondence: Toru Misawa, MD, PhD, Department of Cardiology, Japanese Red Cross Musashino Hospital, 1-26-1 Kyonancho, Musashinoshi, Tokyo, Japan. Email: misawa.toru112@gmail.com
References
1. Ashikaga T, Lee T, Miyazaki R, et al. Methods for treating coronary eruptive calcified nodules. Catheter Cardiovasc Interv. 2024;104(5):899-906. doi:10.1002/ccd.31226
2. Ali ZA, Kereiakes D, Hill J, et al. Safety and effectiveness of coronary intravascular lithotripsy for treatment of calcified nodules. JACC Cardiovasc Interv. 2023;16(9):1122-1124. doi:10.1016/j.jcin.2023.02.015










