Very Late Mechanical Mitral Valve Prosthesis Dehiscence
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00103. Epub April 15, 2026.
A 54-year-old man with a history of hypertension and mechanical mitral valve replacement (MVR) presented with shortness of breath (NYHA III severity) and bilateral pedal edema for the prior 2 months.
He had undergone surgical MVR for symptomatic severe rheumatic mitral stenosis in 2008. Three months post-surgery, he developed prosthetic valve infective endocarditis with severe mitral regurgitation (MR) secondary to paravalvular leak (PVL), necessitating a second MVR. After 2 months of second redo surgery, he presented to the emergency service with prosthetic valve thrombosis requiring a third MVR with a 27-mm St. Jude Medical Regent bi-leaflet mechanical valve (Abbott). Following the lengthy hospital stay, he was healthy on annual follow-up until the current presentation.
At presentation, his jugular venous pressure was elevated, his heart rate was 110 beats per minute with regular pulse, and his respiratory rate was 20 breathes per minute with bi-basal crepitations. Cardiac auscultation revealed a holosystolic murmur with mechanical S1. Laboratory investigations revealed moderate anemia (Hb 9.9 g/dL), elevated serum LDH (1298 U/L), reduced serum haptoglobin, and reticulocytosis. Peripheral blood smear showed schistocytes. Blood cultures were sterile with serum inflammatory markers within normal limits. Electrocardiogram showed sinus tachycardia. He was diagnosed with congestive heart failure with intravascular hemolytic anemia.
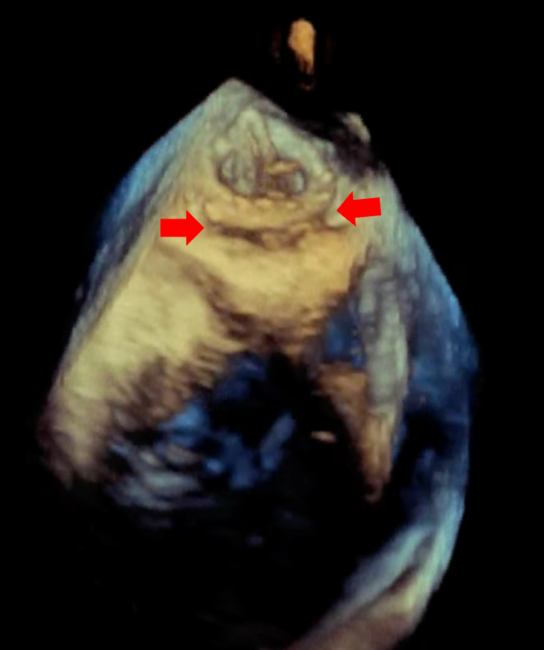
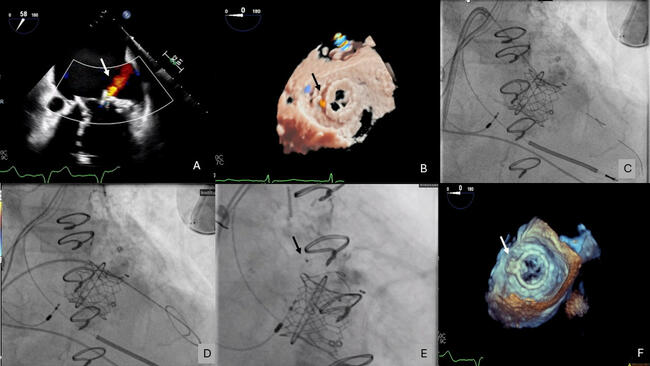
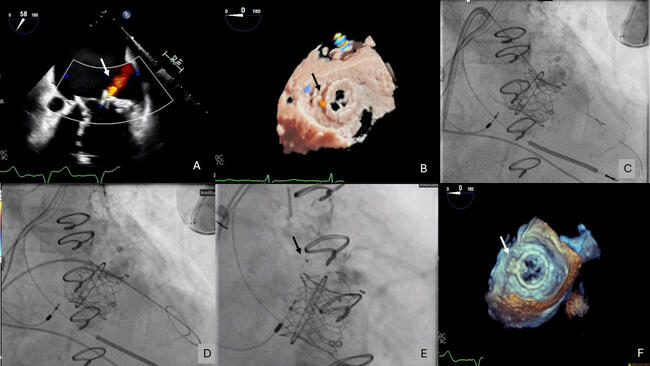
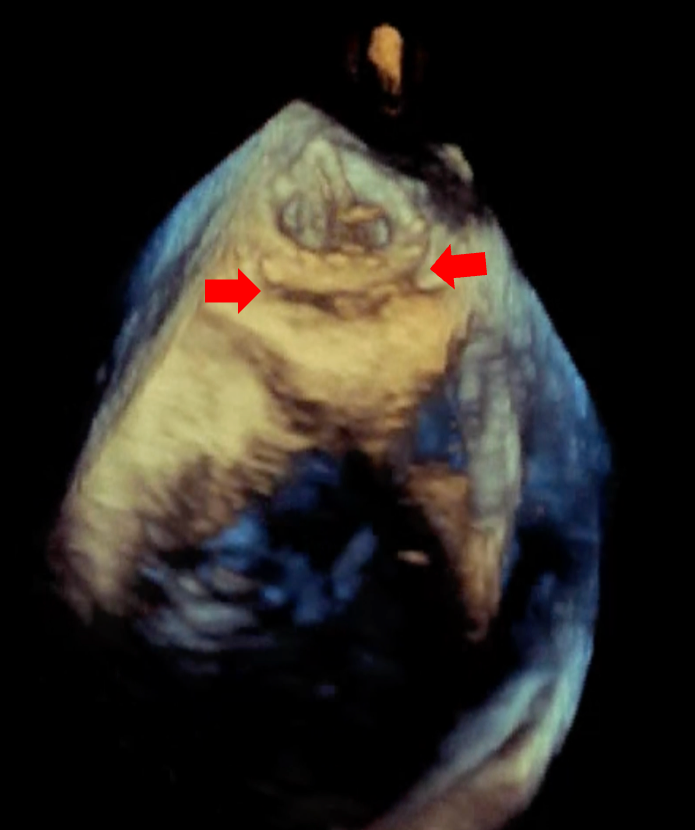
Echocardiography showed severe MR due to PVL with normal biventricular function. No vegetation or perivalvular collection was noted, and the other valves were normal. Transesophageal echocardiography showed a large PVL of the prosthetic mitral valve with valve dehiscence (Figure, Video 1). Coronary angiogram showed complete occlusion of the right coronary artery (RCA). Left ventricular angiography showed Seller grade 4 MR (Video 2) with a relatively small atrium.
Following heart team consultation and discussion of management options with the patient, a plan for redo surgical management of the PVL with coronary bypass graft to the RCA was made. Following the surgery, the patient had a prolonged hospitalization and died after 2 months, secondary to septic shock due to hospital-acquired pneumonia.
PVLs have been described in prosthetic MVRs and occur because of an imperfect seal between the prosthetic valve and surrounding annulus. Risk factors include patient (endocarditis, friable tissue, annular calcium)- and procedure-related factors (mechanical valve and continuous sutures are a greater risk than bioprosthetic valve and interrupted sutures, respectively). Most PVLs are identified in the first year following surgery. Late PVL is usually attributed to infective endocarditis or late resorption of annular calcification, which leads to suture dehiscence.
The present case is unique, with non-infectious prosthetic mitral valve dehiscence occurring 18 years after surgery in a middle-aged man. Extended postoperative monitoring to detect very late PVL, especially in patients with a history of reoperations, and multidisciplinary evaluation with heart team consultation is required for optimal management of these cases.
Affiliations and Disclosures
Shashwat Joshi, MBBS; Shivam Goel, MD, DM; Saurabh Kumar Gupta, MD, DM; Sivasubramanian Ramakrishnan, MD, DM; Sourabh Agstam, MD, DM
From the Department of Cardiology, All India Institute of Medical Sciences, New Delhi, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient(s) for the study and/or intervention(s) described in the manuscript and for the publication of their data/thereof, including any and all images.
Address for correspondence: Sourabh Agstam, MD, DM, MRCP(UK), FACC, Department of Cardiology, 7th Floor, Cardiothoracic Center, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110029, India. Email: sourabhagstam@gmail.com; X: @AgstamSourabh