

Potential Alternative Mechanism of HydroDynamic Contrast Recanalization in Complete Total Occlusion Seen on DeepOCT+NIRS Imaging
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00047. Epub April 16, 2026.
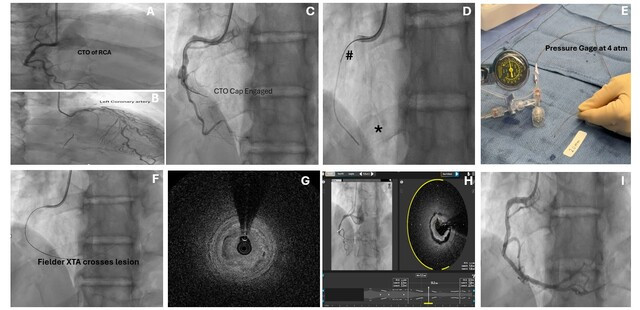
A 69-year-old man was referred for percutaneous coronary intervention (PCI) of a right coronary artery (RCA) in-stent complete total occlusion (CTO) (Figure A), which had collateral supply from the left anterior descending artery (Figure B).
Primary HydroDynamic contrast recanalization (HDR) was performed using a 7F Judkins Right-4 guide catheter (Medtronic). The tip of a Corsair Pro microcatheter (ASAHI INTECC) was advanced into the proximal cap over a 0.14-inch Runthrough wire (Terumo) (Figure C), and was followed by injection of droplets of contrast, utilizing a pressure gauge inflator and limiting the pressure to 4 atm (Figure D and E). Following contrast injection, a 0.14-inch Fielder XTA (ASAHI INTECC) successfully crossed into the distal RCA (Figure F). A DeepOCT+NIRS catheter (SpectraWAVE, Inc.) was then advanced.
Optimal computed tomography revealed that contrast had penetrated inside the plaque of the CTO in a circumferential pattern (Figure G, Video). Predilatation of the lesion with a compliant ballon led to a 360-degree intimal dissection (Figure H, Video); this may be related to the pattern of plaque modulation by HDR leading to injury of structurally weaker areas within the obstruction.
Ultimately, the patient underwent successful PCI of the RCA with a drug-eluting stent (Figure I) and was discharged home.
Affiliations and Disclosures
Arber Kodra, MD; Danyal Khan, MD; Michael Kim, MD; Tak Kwan, MD
From the Department of Cardiology, Northwell Health, Lenox Hill Hospital, New York, New York.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention(s) described in the manuscript and for the publication thereof, including any and all images.
Address for correspondence: Arber Kodra, MD, Department of Cardiology, Northwell Health, Lenox Hill Hospital,100 East 77th Street, 9BH, New York, NY 10075, USA. Email: akodra@northwell.edu













