Closure of Symptomatic Mitral Paravalvular Leak Following Recent Transcatheter Mitral Valve-in-Ring
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00050. Epub April 15, 2026.
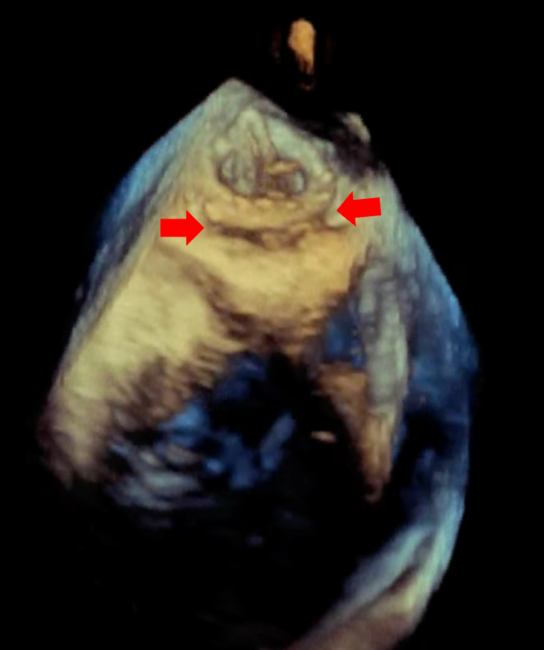
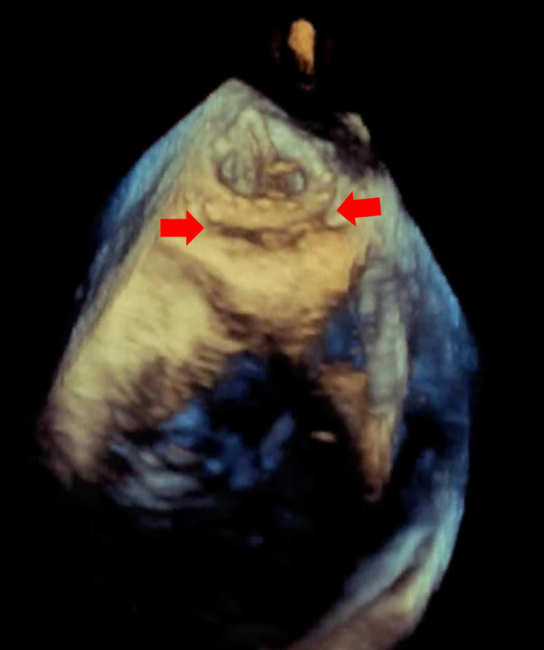
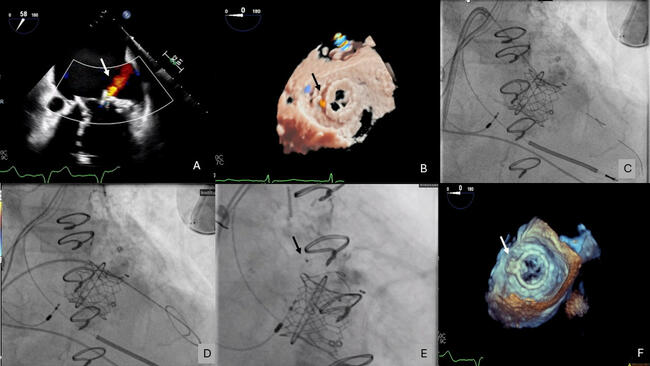
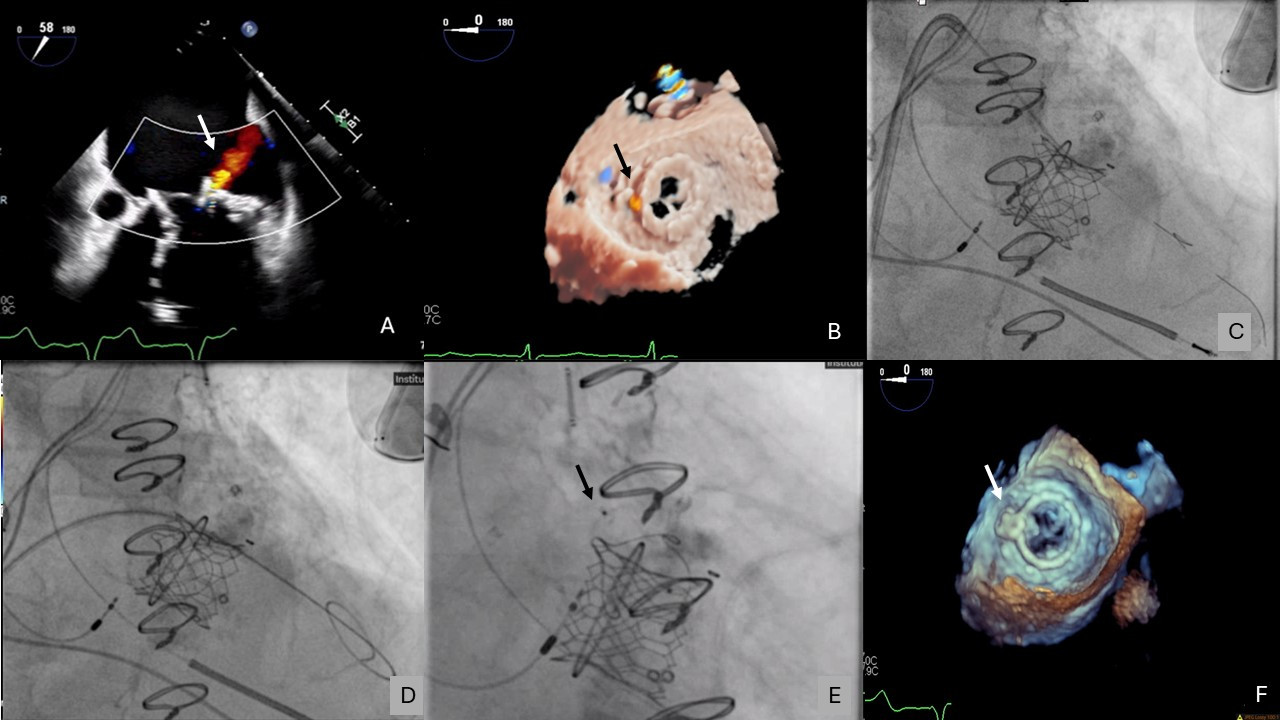
An 86-year-old man who had undergone recent transcatheter mitral valve-in-ring at an outside hospital presented with multiple hospitalizations for symptomatic hemolytic anemia requiring blood transfusions. Transesophageal echocardiogram (TEE) demonstrated mitral paravalvular leak (PVL) originating laterally between the transcatheter valve and surgical ring (Figure 1A and B, Video 1).
The patient underwent transcatheter mitral PVL closure. A 14F Dryseal sheath (Gore Medical) was inserted into the right femoral vein. A catheter was advanced across the pre-existing atrial septal defect into the left atrium and was exchanged for an 8.5F Agilis sheath (Abbott) over a Confida wire (Medtronic). A 6F multipurpose catheter, a 4F angled glide catheter, and an angled Glidewire (Terumo) were advanced into the Agilis.
The Glidewire successfully crossed the PVL and advanced into the left ventricle (LV), but the 4F angled glide catheter could only partially cross the defect. The angled Glidewire was exchanged for 2 Grand Slam coronary wires (ASAHI INTECC) (Figure 1C). The 4F angled glide catheter was exchanged for a 5F tapered catheter, which was successfully advanced into the LV. The Grand Slam wire was exchanged for the Confida wire (Video 2).
The 6F multipurpose catheter could not advance across the PVL. The 8.5F Agilis and 6F multipurpose catheters were exchanged for a Flexor Shuttle sheath (Cook Medical), which also could not cross the PVL. A 6F Radial to Peripheral (R2P) sheath (Terumo) was successfully advanced across the PVL (Figure 1D). A 6 x 6-mm Amplatzer Duct Occluder II (ADO II) (Abbott) was advanced through the R2P sheath and deployed. After TEE demonstrated significant reduction in the PVL, the Confida wire was retracted into the R2P sheath and the device was released (Figure 1E, Video 3).
Postprocedural TEE demonstrated complete resolution of the PVL (Figure 1F, Video 4). The patient was discharged home the following day with stable hemoglobin at follow-up.
This case illustrates that symptomatic mitral PVL can be safely and successfully treated using the R2P sheath/guiding catheter and an ADO II plug.
Affiliations and Disclosures
Matthew Atienza, MD1; Ahmad Alkhalil, MD1; Neda Dianati Maleki, MD1; Jonathan Price, MD2; Daniel Montellese, MD1; Puja Parikh, MD1
From the Departments of 1Medicine and 2Surgery, Stony Brook University Hospital, Stony Brook, New York.
Disclosures: Dr. Alkhalil serves as a speaker for Abbott and Medtronic, Inc. Dr Parikh is a consultant for Medtronic, Inc., and has received institutional research support from Edwards Lifesciences and Abbott. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the interventions described in this manuscript and for the publication of their data.
Address for correspondence: Puja B. Parikh, MD, MPH, FACC, FAHA, FSCAI, Division of Cardiovascular Medicine, Stony Brook University Renaissance School of Medicine Health Sciences Center T16-080, Stony Brook, NY 11794, USA. Email: puja.parikh@stonybrookmedicine.edu