Fibrillatory Left Atrial Appendage With Tip Clot
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2025. doi:10.25270/jic/26.00015. Epub February 11, 2026.
A 54-year-old woman with rheumatic heart disease and percutaneous transvenous mitral commissurotomy (PTMC) 15 years prior presented with worsening dyspnea (New York Heart Association class II-IV) for a duration of 3 months. The patient had been on warfarin for atrial fibrillation (AF), beta blockers, and diuretics over the last 3 months from our outpatient department.
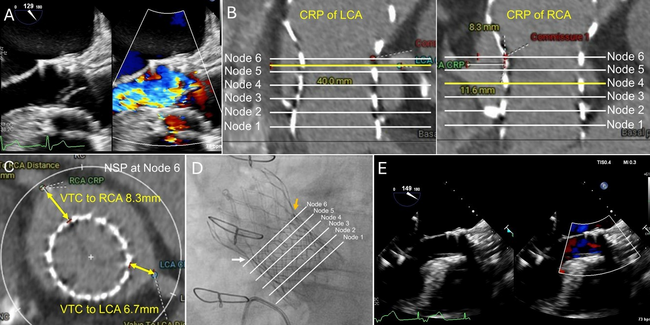
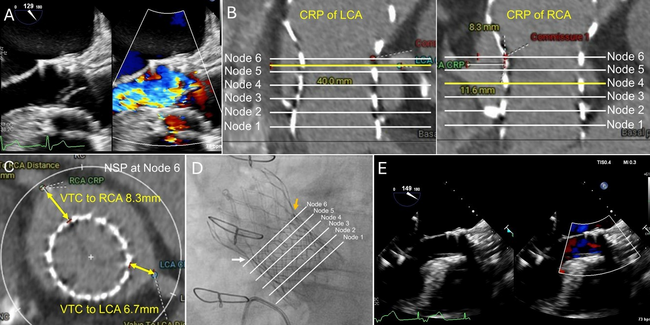
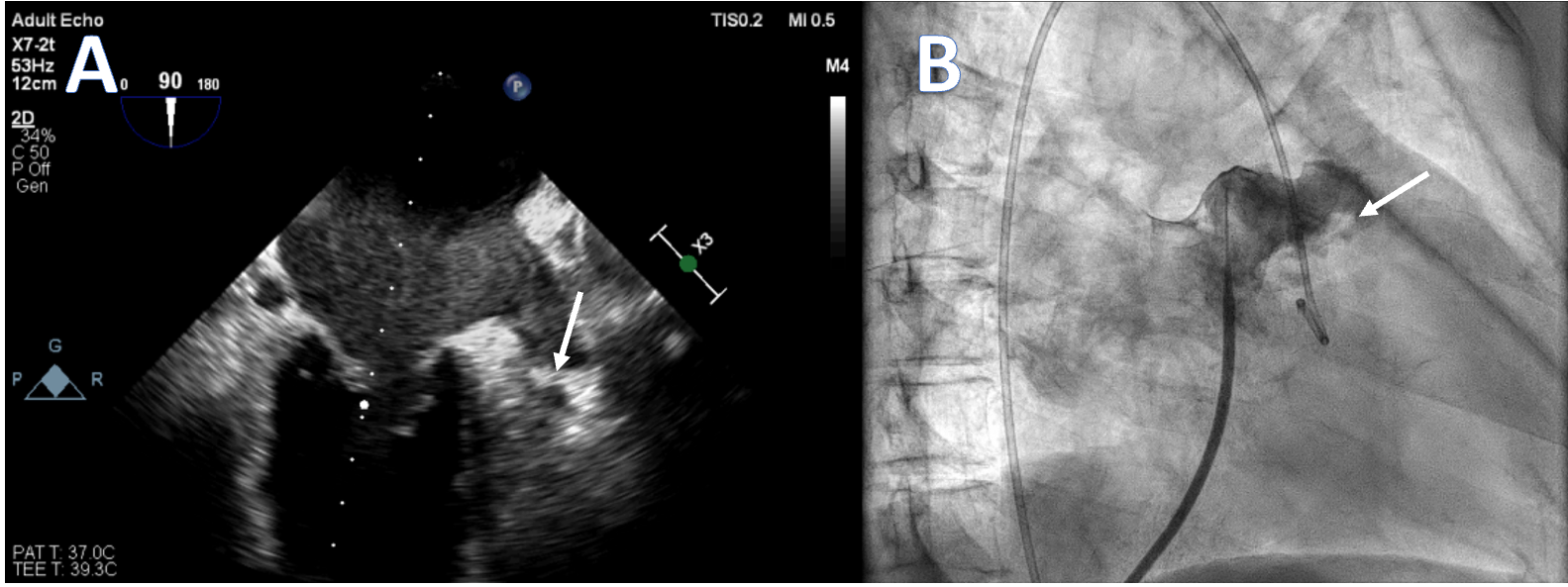
She was tachypneic upon examination, and diffuse wheezing was present on lung auscultation. The 12-lead electrocardiogram showed AF with a fast ventricle rate. Transthoracic echocardiography showed severe mitral restenosis (mitral valve area: 1.0 cm² [normal 4-6 cm2]) and reduced left ventricular function, likely due to persistent AF. Transesophageal echocardiography revealed spontaneous echo contrast in the left atrium and an organized thrombus in the left atrial appendage (LAA) tip (Manjunath Type 1a) (Figure A). In view of worsening symptoms, patient was initially stabilized and a redo PTMC was planned. During hospital stay, the warfarin was stopped and bridging with low-molecular-weight heparin was initiated.
After septal puncture, intraprocedural intravenous unfractionated heparin was given. The LA angiography demonstrated a dilated and fibrillating appendage with a "quivering" motion. A distinct area of haziness and a contrast-unfilled defect were visualized at the appendage tip (Figure B, Video). The PTMC was done with utmost care to prevent the movement of the balloon to the LAA appendage, and the mitral valve area increased to 1.8 cm².
This case has unique educational value, illustrating a fibrillatory LAA appendage, dynamic angiographic appearance of LAA stasis, and the importance of anticoagulation. The patient was discharged on warfarin with frequent monitoring of her international normalized ratio, and lifelong anticoagulation was recommended for management of her AF. This case demonstrates that with careful case selection and cautious catheter manipulation, PTMC remains feasible in high-risk anatomies.
Affiliations and Disclosures
Rakavi Rathinasamy, MD, DM; Sunil Solan, MD; Gautam Sharma, MD, DM; Sourabh Agstam, MD, DM
From the Department of Cardiology, All India Institute of Medical Sciences, New Delhi, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and for the publication thereof, including photographs.
Address for correspondence: Sourabh Agstam, MD, DM, MRCP(UK), FACC, Department of Cardiology, 7th Floor, Cardiothoracic Center, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110029, India. Email: sourabhagstam@gmail.com