

Measuring Justice in Breast Cancer Screening: A Bioethical Framework for Analyzing Quality Measures
The predominant US health care quality measure development and endorsement processes, as summarized in the Centers for Medicare and Medicaid Services (CMS) Blueprint, define various well-accepted criteria for evaluating measures. In this blog series, we will view quality measure evaluation through the lens of bioethical principles, using oncology measures as examples. While bioethical principles are fundamental to all health care practices, they are not formally prioritized during quality measure development. This third and final blog in the series will apply the principle of justice to analyze the Breast Cancer Screening quality measure. The first blog in our series addressed the principles of beneficence and nonmaleficence; the second addressed the principle of autonomy.
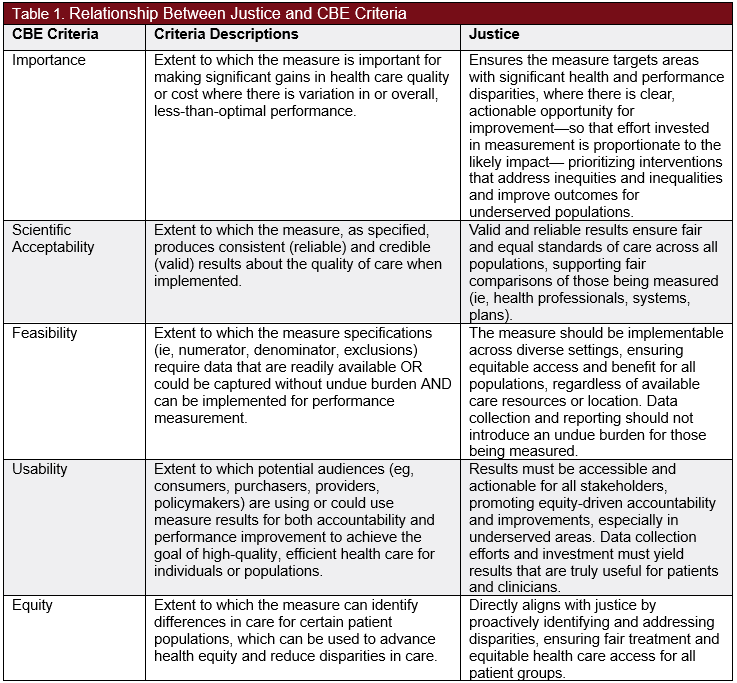
In Principles of Biomedical Ethics, bioethicists Beauchamp and Childress describe the principles of beneficence, nonmaleficence, autonomy, and justice to collectively form a framework for analyzing ethical issues in health care. The current federal Consensus-Based Entity (CBE), the Partnership for Quality Measurement (PQM), is responsible for endorsing quality measures and applies specific criteria of importance, scientific acceptability, feasibility, usability, and equity to evaluate measures. In particular, the equity and usability criteria overlap somewhat with the bioethical principle of justice (Table 1). Although the PQM’s endorsement criteria implicitly touch on components of the 4 bioethical principles, an intentional ethical perspective would provide insight into how quality measures serve public health, enhance quality of care, and improve patient outcomes.
Justice
The principle of justice pertains to the fair distribution of health care resources. In this context, it is crucial to differentiate between equity and equality and understand their significance. Equality generally refers to offering individuals or groups the same level of resources or access, whereas equity involves providing resources in proportion to individuals’ or groups’ differing needs to achieve fair outcomes. The principle of justice is typically interpreted in equity-oriented terms: Individuals should have access to needed medical services that are fair considering their health needs and circumstances rather than identical in amount. At the same time, justice also requires equal respect and non-discrimination, so that no one is disadvantaged based on socioeconomic status, race, ethnicity, or geographic location. Justice in health care not only involves fair allocation of resources according to need, but also the recognition and rectification of disparities that exist within health care systems, ensuring that health care practices promote equal opportunities for all to achieve optimal health outcomes.
Justice is often challenged by structural and systemic inequities that have led to inequitable distribution of care resources. Beyond treatment, access extends to addressing financial constraints, transportation issues, and cultural/language differences. Justice requires first a commitment to identifying access and resource barriers, and second, the implementation of policies that remove barriers for marginalized populations to ensure that individuals have equitable access to resources for care that is responsive to need.
Beyond justice for individuals as patients, the principle of justice must also consider fairness in accountability for those providing services and being measured. Quality measure specifications, data collection, and other factors like risk adjustment must be fair and beneficial to all parties involved, including accountable entities such as health professionals, systems, and plans, as well as patients.
Breast Cancer Screening Measure
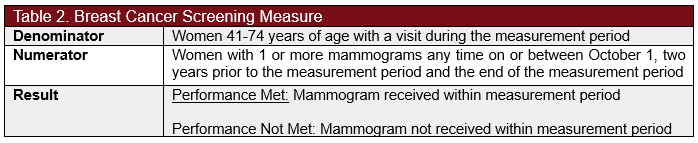
The Breast Cancer Screening measure (Table 2), developed by the National Committee for Quality Assurance (NCQA), evaluates the percent of women aged 41-74 years who receive 1 or more mammograms within each measurement period. Breast cancer is the one of the most prevalent cancers among women in the US, accounting for about 30% of all new female cancers annually. The American Cancer Society estimates that in 2025, there will be approximately 316 950 incident cases of invasive breast cancer, 59 080 new cases of ductal carcinoma in situ (DCIS), and 42 170 deaths due to breast cancer. The median age at diagnosis is 62 years, with a lifetime risk of 13% for women. Annual breast cancer screening is critical for early disease detection.
Measure Analysis: Breast Cancer Screening
It is critical that breast cancer screening is promoted for high-risk women, as well as for minority women who often receive lower rates of screening, diagnosis, and care. Research indicates that non-Hispanic White women have the highest breast cancer diagnosis rates, followed by Black, Asian and Pacific Islander, Hispanic, and American Indian and Alaska Native women. Black women are often diagnosed at later stages, when disease has become more aggressive, complicating treatment. Likewise, recent studies show rising breast cancer incidence in Black and Asian and Pacific Islander women, while rates remain stable in other groups. White women are also more likely to be diagnosed with breast cancer, though Black women are more likely to die from the disease. Additional evidence of disparities shows that supplemental breast imaging is less likely to be ordered for minority women with dense breasts. The U.S. Preventive Services Task Force has noted these disparities, calling for evidence development and research to address them. These recognized disparities underscore a critical need to improve access to breast cancer screening and earlier treatment for high-risk minority women.
Besides racial disparities, there are several other barriers to justice that complicate breast cancer screening access. Socioeconomic disparities significantly reduce access to screening. One study found that women with lower levels of education and household income reported missing mammography screenings at higher rates. Additionally, self-employed women were the most likely to skip mammograms. Demographic factors such as geographic location and socioeconomic status may highlight cohorts of women who do not routinely receive screening and likely other critical care. Geographic conditions similarly impede screening, with women in rural areas accessing mammography screening at lower rates than their urban counterparts.
Besides these patient-centered barriers, there are also barriers within health systems that create new obstacles and exacerbate others. A study on integrating breast cancer screening into primary care found that women on high genetic-risk pathways (eg, genetic predisposition to BRCA2 gene) faced barriers such as limited clinician knowledge about risk assessment and specialist services, as well as unclear referral processes to genetics or breast clinics. For women on low genetic-risk pathways, challenges included clinician reluctance to adopt new screening models, inconsistencies in how guidelines were interpreted and applied in practice, and difficulties communicating risk information in ways that patients could understand and use. These concerns also highlight whether mammography services are distributed in ways that genuinely reach all patients at risk, rather than primarily serving those with the easiest access. Measure evaluators should assess whether the measure is structured to avoid favoring one group over another and, where possible, explicitly incorporate mechanisms to promote equitable access to screening across different populations.
While the barriers discussed above are significant, they are just a few of the factors affecting high-quality, equitable breast cancer screening. It is critical that quality measure developers and policymakers consider and address disparities and ensure that care is delivered in an equitable manner. This means that in efforts to enhance access to care for at-risk and high-risk patients, measures should be implemented to ensure necessary care is accessible to all, not just those with advantages that enable easier access. To promote justice in breast cancer screening, quality measurement should be structured to promote equitable access to care across demographics of patients, holding health professionals, systems, and plans accountable for addressing access barriers.
In addition to patient-facing fairness, there are also important fairness considerations for those being measured. Collecting and reporting data for the breast cancer screening measure can create a substantial burden for clinicians, health systems, and plans, particularly when data elements are not easily captured electronically. Moving toward electronic measures and better integration with existing health information systems could reduce manual reporting, decrease administrative workload, and improve data quality. In addition, the usefulness of measurement results for clinicians and plans must justify this burden: Results should be timely, actionable, and clearly linked to potential improvements in patient care. Professionals should be responsible for identifying eligible patients, recommending appropriate screening, and reducing modifiable barriers within the clinical setting. They cannot reasonably be held fully accountable for broader demographic factors or for patients’ personal decisions about accessing medical care. Fair use of breast cancer screening measure data should recognize both the obligation to promote equitable access to screening and the practical constraints faced by those whose performance is being evaluated.
Opportunities for Enhancement
To effectively identify opportunities to improve the Breast Cancer Screening measure, it is important to analyze how its components align with the subprinciples of justice, as well as to identify any existing gaps (Table 3).
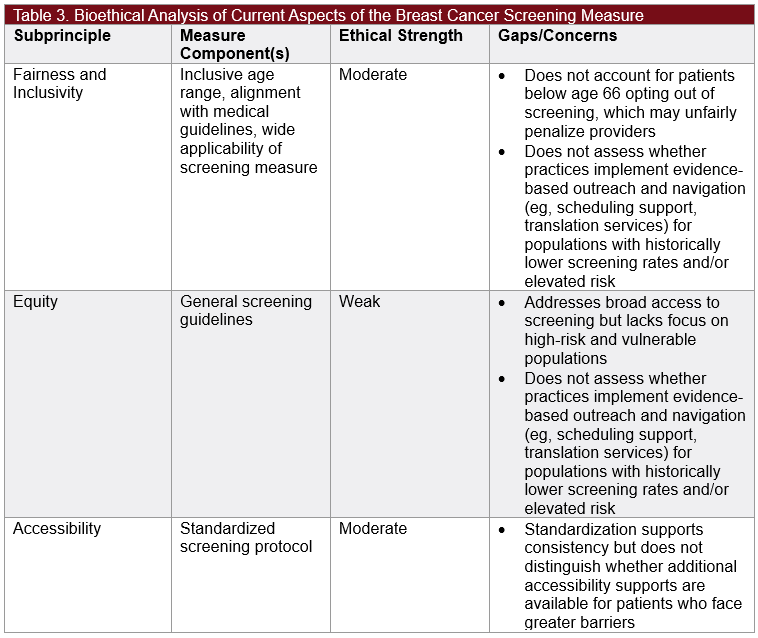
Our evaluation of the Breast Cancer Screening measure indicates that enhancements can be made by expanding reporting criteria (eg, outreach improvements and capture of opt-outs) to better align with the principle of justice. For example, the measure could include stratification by high-risk status, involving subsequent annual or increased screenings for eligible patients. This refinement would incentivize greater focus on high-risk individuals, enabling more meaningful improvements in patient outcomes, ensuring earlier diagnoses, and addressing current disparities among high-risk women across demographic groups.
Likewise, the current measure does not adequately support clinicians and health systems in identifying and monitoring whether there is an equitable distribution of care across vulnerable populations that experience barriers to screening. The measure could incorporate race and ethnicity stratification, socioeconomic indicators, and other critical demographic information into required data collection to better understand which women receive mammography screening and where disparities exist. Increased data collection, ideally through electronic reporting, could then uncover further insights into the breadth and fairness of care, identifying gaps that clinicians and health systems can address. Conversely, the measure does not fairly exclude all patients who are eligible for screening but who choose to opt out against clinicians’ advice. Including these patients in performance calculations may lead to unfair penalties for clinicians who have otherwise been diligent in identifying and recommending patients for screening.
Conclusion
This analysis of the Breast Cancer Screening measure illustrates how the principles of a bioethical framework can be applied to assess quality measures, particularly through the lens of justice. This principle highlights the importance of promoting fairness, inclusivity, and equity to patients who are eligible for screening, as well as the entities being measured and held accountable for performance. By integrating an ethical framework into quality measure analysis, measure developers and implementers can enhance the effectiveness of quality measures in addressing health outcomes and meeting patient needs.
 About Nandita Ammanamanchi, BA
About Nandita Ammanamanchi, BA
Nandita Ammanamanchi is a senior analyst on the Real-World Data team at Real Chemistry, where she applies her expertise in health care research, health equity, and data analytics to inform strategic decision-making across therapeutic areas. She is currently pursuing a Master of Science in Bioethics at Harvard Medical School, with a capstone focus on narrative ethics in high-intensity care settings. Nandita brings a multidisciplinary lens to complex challenges in health care policy and access. She is passionate about leveraging data and research to drive equitable health outcomes and shape the future of health care.
 About Rachel Delinger, MPH
About Rachel Delinger, MPH
Rachel Delinger is a director on the Real Chemistry Real-World Data team. She is data-driven with expertise in outcomes research and real-world evidence generation and works across functions to inform market access strategy. She serves as a quantitative methodologist and supports evidence generation efforts that align with evolving access landscapes. She brings a strong analytical foundation to market access strategy, bridging clinical, economic, and patient-centered perspectives.

About David Blaisdell, BA
David Blaisdell is a value-based care subject matter expert, providing insight on quality landscape analyses and measure gap identification. David formerly led and contributed to Real Chemistry Market Access projects focused on oncology quality measurement to identify key gaps in measures used in accountability programs and opportunities for measure development. Through this experience, David helped clients navigate measurement and value-based payments and define strategies for success.
 About Tom Valuck, MD, JD
About Tom Valuck, MD, JD
Tom Valuck, MD, JD, is the editor of Quality Outlook. He formerly led the Value-Based Care discipline for the Market Access team at Real Chemistry. He used research and strategic advisory services to help clients improve health and health care by assessing, responding to, and shaping the value landscape.
Tom is a thought leader on health care system transformation, focused on achieving better health and health care outcomes at a lower cost. His work includes facilitating the exploration of next-generation measurement and accountability models for health care delivery systems. He also helps clients develop strategies to achieve success within the value-based marketplace.



