


Sex Differences in Reverse Remodeling After Transcatheter Aortic Valve Replacement in Low-Flow Aortic Stenosis
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00117. Epub June 22, 2026.
Abstract
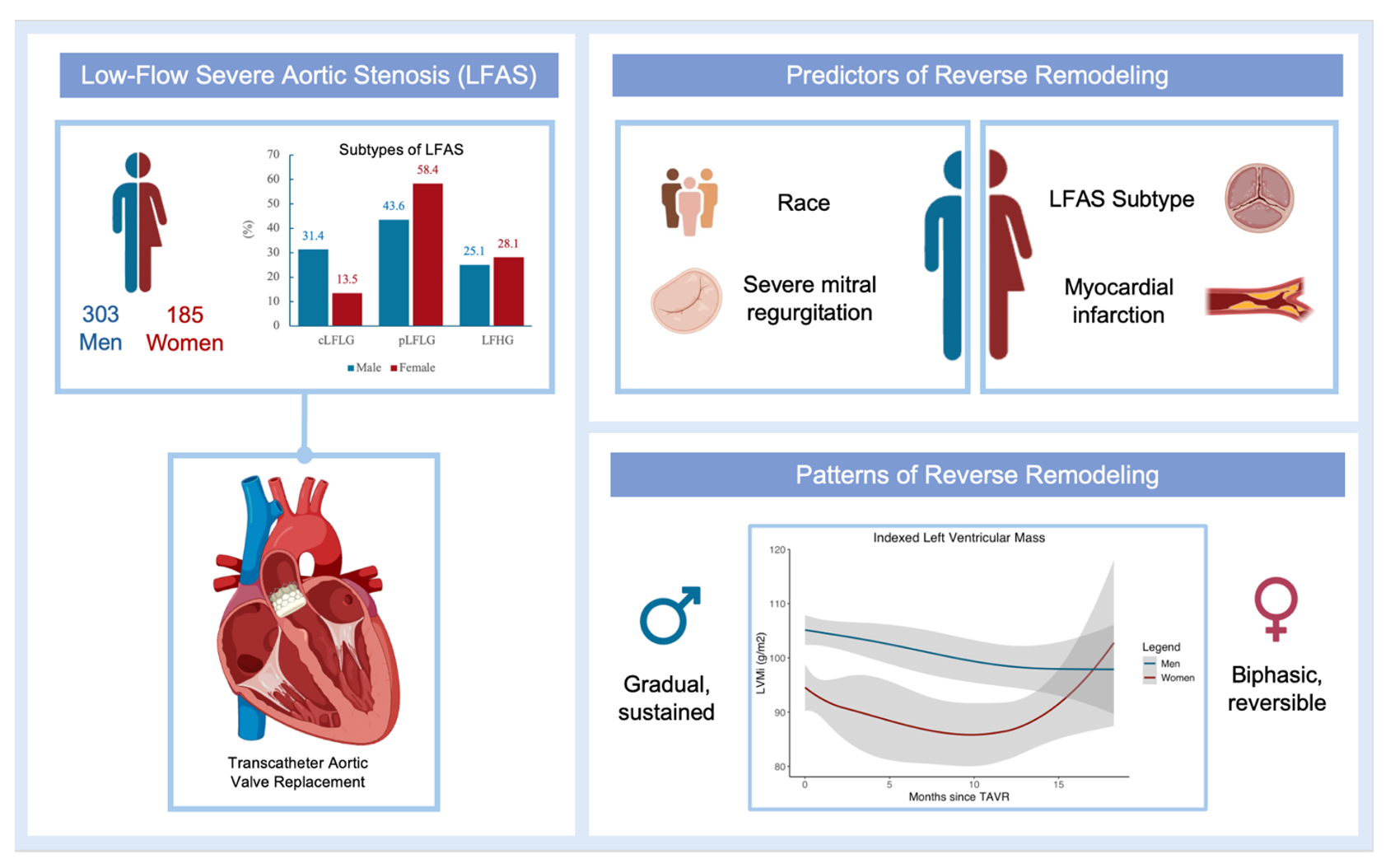
Objectives. Sex-specific differences in left ventricular (LV) remodeling after transcatheter aortic valve replacement (TAVR) in low-flow aortic stenosis (LFAS) remain incompletely defined, and the influence of LFAS subtype on remodeling by sex is uncertain. The authors sought to characterize post-TAVR remodeling in LFAS by sex and subtype and identify predictors of remodeling.
Methods. This retrospective cohort study included 488 patients with LFAS (303 men, 185 women) who underwent TAVR. Smoothed conditional mean curves assessed longitudinal changes in LV mass index (LVMi), relative wall thickness (RWT), and LV ejection fraction (LVEF) through 18 months. Linear mixed models identified predictors of remodeling.
Results. Women more often had paradoxical low-flow low-gradient (pLFLG) AS (58.4% vs 43.6%, P = .001), whereas men more often had classical low-flow low-gradient AS (31.4% vs 13.5%, P < .001). At 1 year, both sexes showed significant improvement in LVMi, RWT, and LVEF. Men demonstrated sustained improvement in LVEF and LVMi during follow-up, whereas women showed earlier improvement followed by decline beginning around 12 months. Predictors also differed: lower LVMi after TAVR was associated with White race and less severe baseline mitral regurgitation in men, and with pLFLG subtype in women.
Conclusions. Reverse remodeling after TAVR occurred in both sexes, but trajectories and predictors were sex-specific.
Introduction
Current practice guidelines support the role of transcatheter aortic valve replacement (TAVR) for the treatment of symptomatic severe aortic stenosis (AS) across the entire surgical risk spectrum.1,2 Left ventricular (LV) remodeling occurs after TAVR with impact on clinical outcomes.3 LV response to systolic pressure overload is highly heterogeneous, and also varies by the severity of AS, age, history of hypertension, coronary artery disease (CAD), and mitral regurgitation (MR).4 Additionally, LV remodeling differs by sex, ie, men are more likely to develop concentric remodeling and LV dysfunction, while women are more likely to experience concentric hypertrophy without LV dysfunction.3 Overall, the impact of sex on reverse remodeling after TAVR is less conclusive.2-7
While outcomes after TAVR have been extensively studied in various patient populations, the impact of sex on cardiac remodeling post-TAVR, particularly in the context of low-flow aortic stenosis (LFAS), remains incompletely understood. LFAS encompasses several distinct hemodynamic patterns, each presenting unique challenges in diagnosis and treatment. Classical low-flow low-gradient AS (cLFLG AS) is characterized by reduced LV ejection fraction (LVEF) (<50%), low flow (stroke volume index [SVi] <35 mL/m²), and low mean gradient (MG) (<40 mm Hg) despite a small aortic valve area (AVA) (≤1.0 cm²) or indexed AVA (AVAi) (≤ 0.6 cm²/m²). In contrast, paradoxical low-flow low-gradient AS (pLFLG AS) is characterized as preserved LVEF (≥50%) but still exhibits low flow and low gradient. A third category, low-flow, high-gradient AS (LFHG AS), features low flow, but maintains a high MG (≥40 mm Hg). These subtypes not only differ in their underlying pathophysiology, but may also respond differently to TAVR, particularly in the context of sex-specific factors.
Prior studies suggest LFAS in general is associated with worse outcomes after TAVR.8 These outcomes seem to be further modified by subtype of LFAS, with the greatest mortality in the cLFLG group, followed by pLFLG, and finally LFHG AS.9
The aim of this study is to characterize longitudinal cardiac remodeling, as assessed by changes in LV mass index (LVMi), relative wall thickness (RWT), and LVEF, following TAVR in patients with LFAS, and to identify clinical and echocardiographic predictors of these remodeling trajectories. We further aim to determine whether patterns of remodeling and their determinants differ according to sex and LFAS subtype, recognizing that these factors may have distinct pathophysiologic implications for long-term outcomes.
Methods
Study population
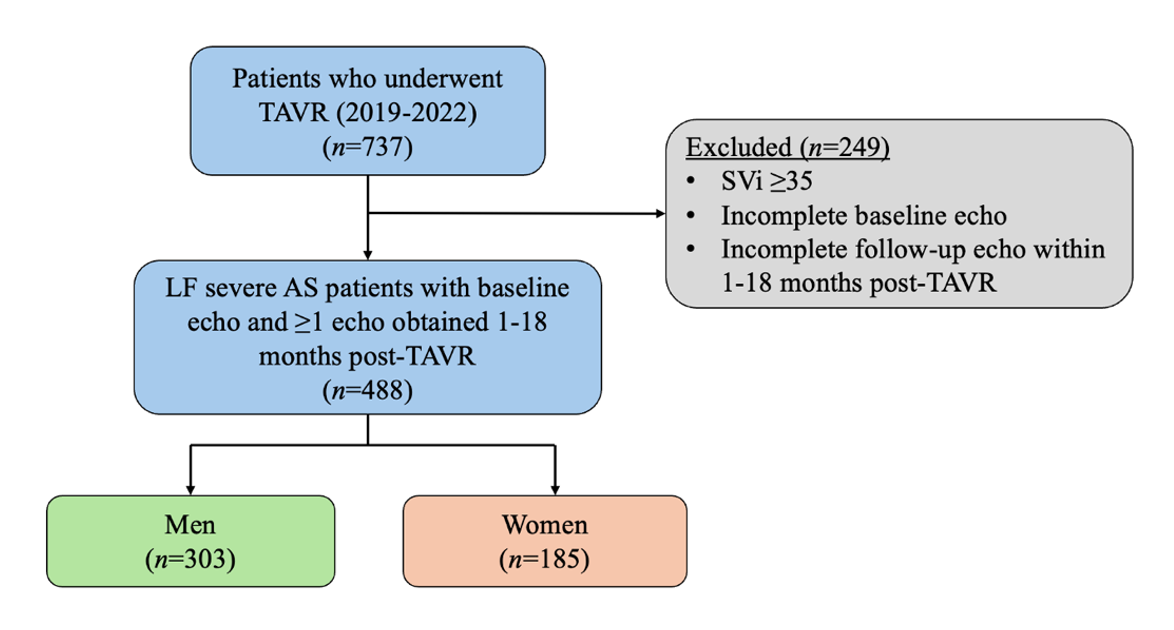
This single-center, retrospective, longitudinal cohort study included consecutive adults with LFAS who underwent TAVR between 2019 to 2022. The study was approved by the Mount Sinai Hospital Institutional Review Board. Prior to TAVR, clinical and demographic data were collected, and all patients received baseline comprehensive 2-dimensional transthoracic echocardiography (TTE). A flow chart summarizes the study in Figure 1. Inclusion criteria were an AVA of less than or equal to 1.0 cm2, an SVi of less than 35 mL/m2, and at least 1 follow-up TTE performed within 1 to 18 months following TAVR. This follow-up interval was selected to capture both early and intermediate-term LV remodeling after afterload reduction. Up to the first 3 follow-up TTEs within the 18-month post-TAVR window were included in the longitudinal analysis. All 488 patients had at least 1 follow-up TTE, and 322 patients (66.0%) had more than 2 follow-up TTEs, enabling longitudinal trajectory estimation. LVMi, RWT, and LVEF were selected to represent changes in LV morphology and function. Patients without these measurements at baseline or at any follow-up time point were excluded from the analysis.
Demographic, clinical, and echocardiographic data
Demographic and clinical data were extracted via retrospective medical record review. Echocardiographic parameters were measured according to American Society of Echocardiography guidelines.10 The following variables were included: peak aortic jet velocity (Vmax), peak aortic gradient (PG), MG, SVi, and AVAi of the native valve at baseline; indexed effective orifice area (EOAi) of the prosthetic valve at follow-up; and LVEF, LV end diastolic diameter (LVEDD), LV end systolic diameter (LVESD), interventricular septal thickness (ST), posterior wall thickness (PWT), LVMi, aortic regurgitation (AR), MR, and tricuspid regurgitation (TR). RWT was calculated from the PWT and LVEDD. Subtype of LFAS was defined for cLFLG, pLFLG, and LFHG.
Outcome
The outcome assessed was longitudinal echocardiographic changes (LVEF, LVMi, and RWT) by sex and subtype of LFAS.
Statistical analysis
Continuous variables were tested for normality with the Shapiro-Wilk test and summarized as mean and standard deviation (SD). Categorical variables were summarized as n and percentage. Differences between sexes were assessed using the Mann-Whitney U test for continuous variable and chi-squared analysis for categorical variables.
Longitudinal changes of LVMi, RWT, and LVEF were visualized using plots of smoothed conditional means, illustrating average trajectories from baseline echocardiography (time = 0 months) to follow-up assessments (up to 18 months). These parameters were also compared between baseline echocardiography and 1-year follow-up using the Wilcoxon signed-rank test. Plots and analyses were performed by sex and subtype of LFAS.
Linear mixed-effect models were constructed to identify variables associated with longitudinal changes in the LVMi, RWT, and LVEF in each sex. Fixed effects included the baseline clinical and echocardiographic variables. Random effects included individual intercepts and slopes for each patient. Variables included in the final models were selected via automated backward selection based on the lowest Akaike Information Criterion. A sex × LFAS subtype interaction term was included. All analyses were performed with R statistical software, version 4.3.2 (R Foundation for Statistical Computing).
Results
Baseline clinical and echocardiographic characteristics
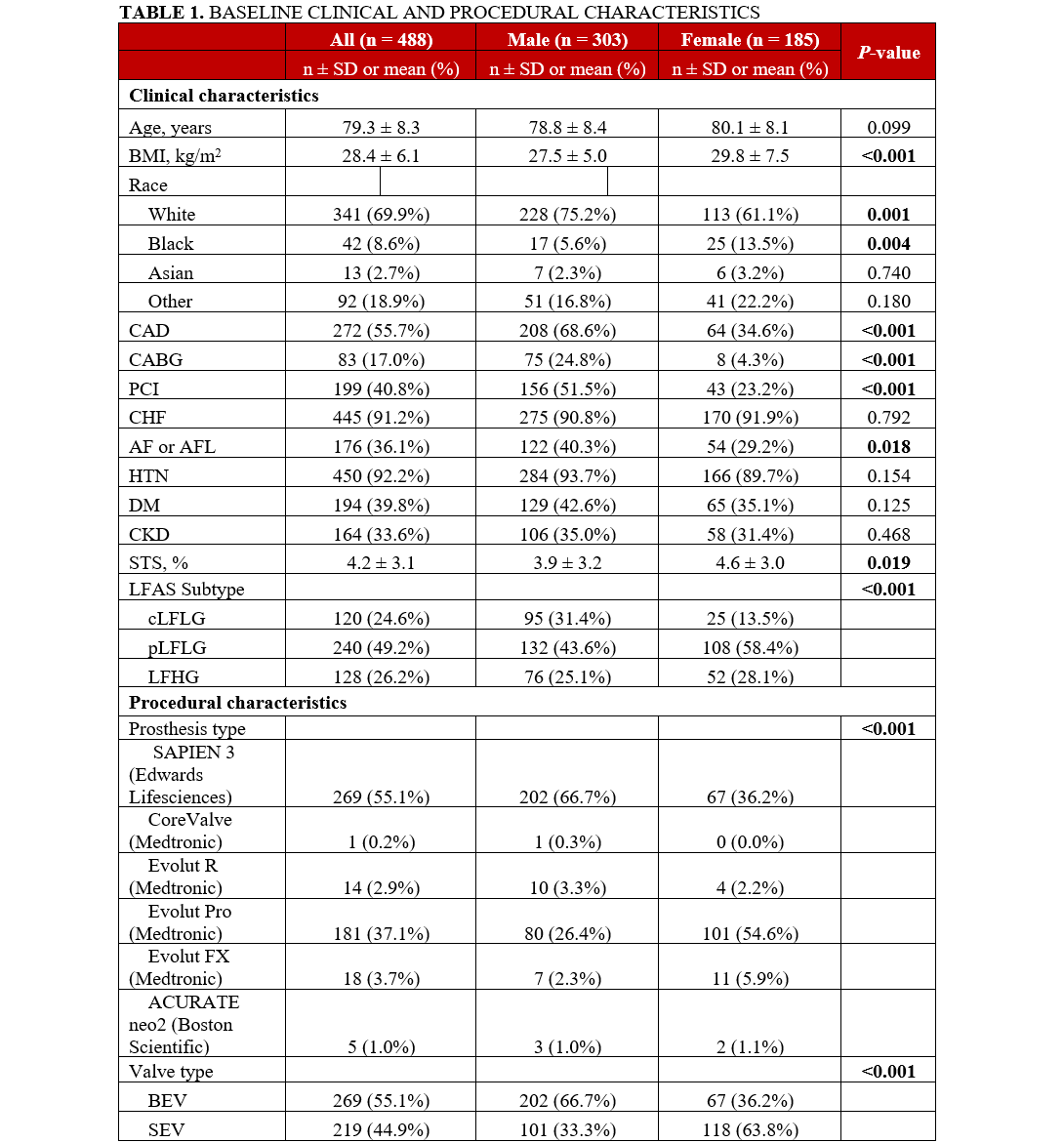
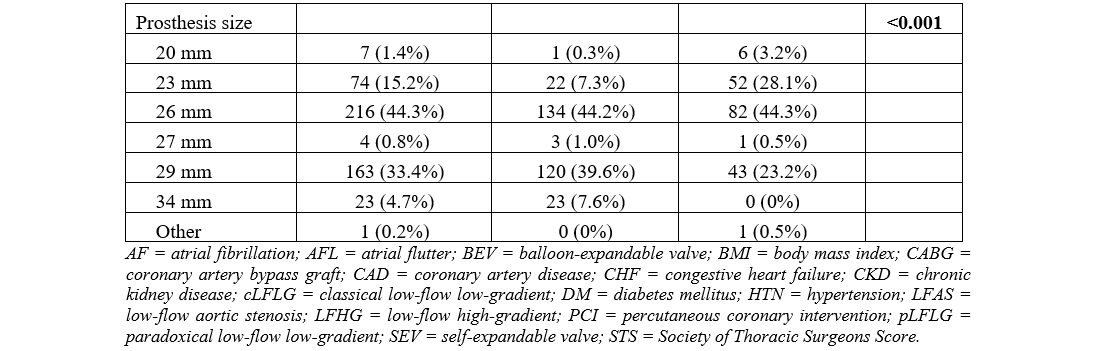
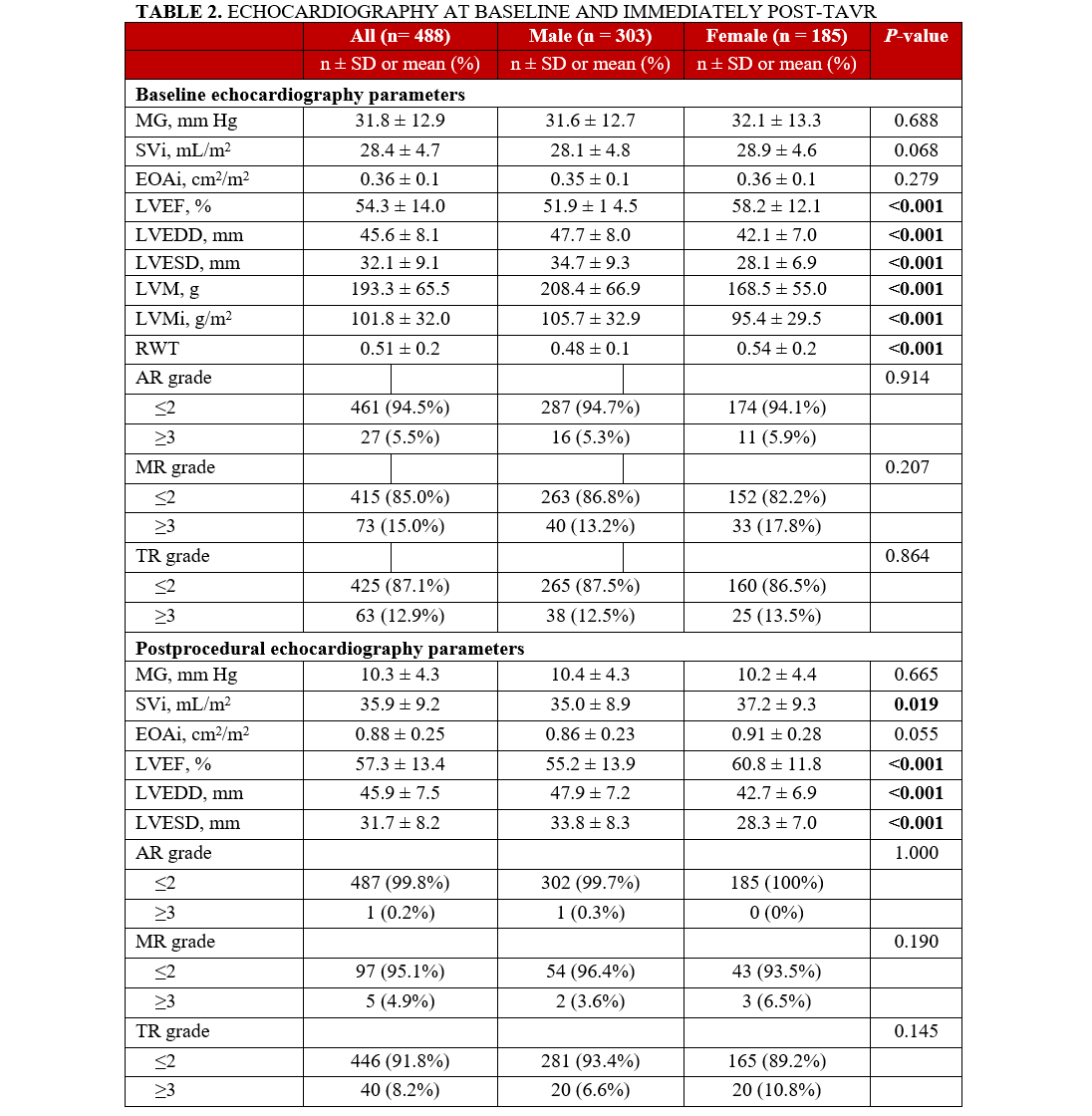
A total of 488 patients who underwent TAVR were included in this study. Of these, 303 (62.1%) were men and 185 (37.9%) were women. Baseline clinical and echocardiographic characteristics are summarized in Tables 1 and 2. Compared with women, men had significantly higher prevalence of atrial arrhythmias, coronary disease, and coronary interventions, but lower Society of Thoracic Surgeons (STS) scores at baseline. The distribution of subtypes of LFAS differed significantly between sexes. More than half (58.4%) of women had pLFLG, followed by LFHG (28.1%), and cLFLG (13.5%) AS. In men, the distribution was 43.6% pLFLG, 31.4% cLFLG, and 25.1% LFHG AS. Balloon-expandable valves (BEV) were more likely to be used in men, while self-expandable valves (SEV) were more likely to be used in women. Men had lower baseline LVEF and RWT, but higher LVMi compared with women.
Longitudinal changes in LV geometry and function
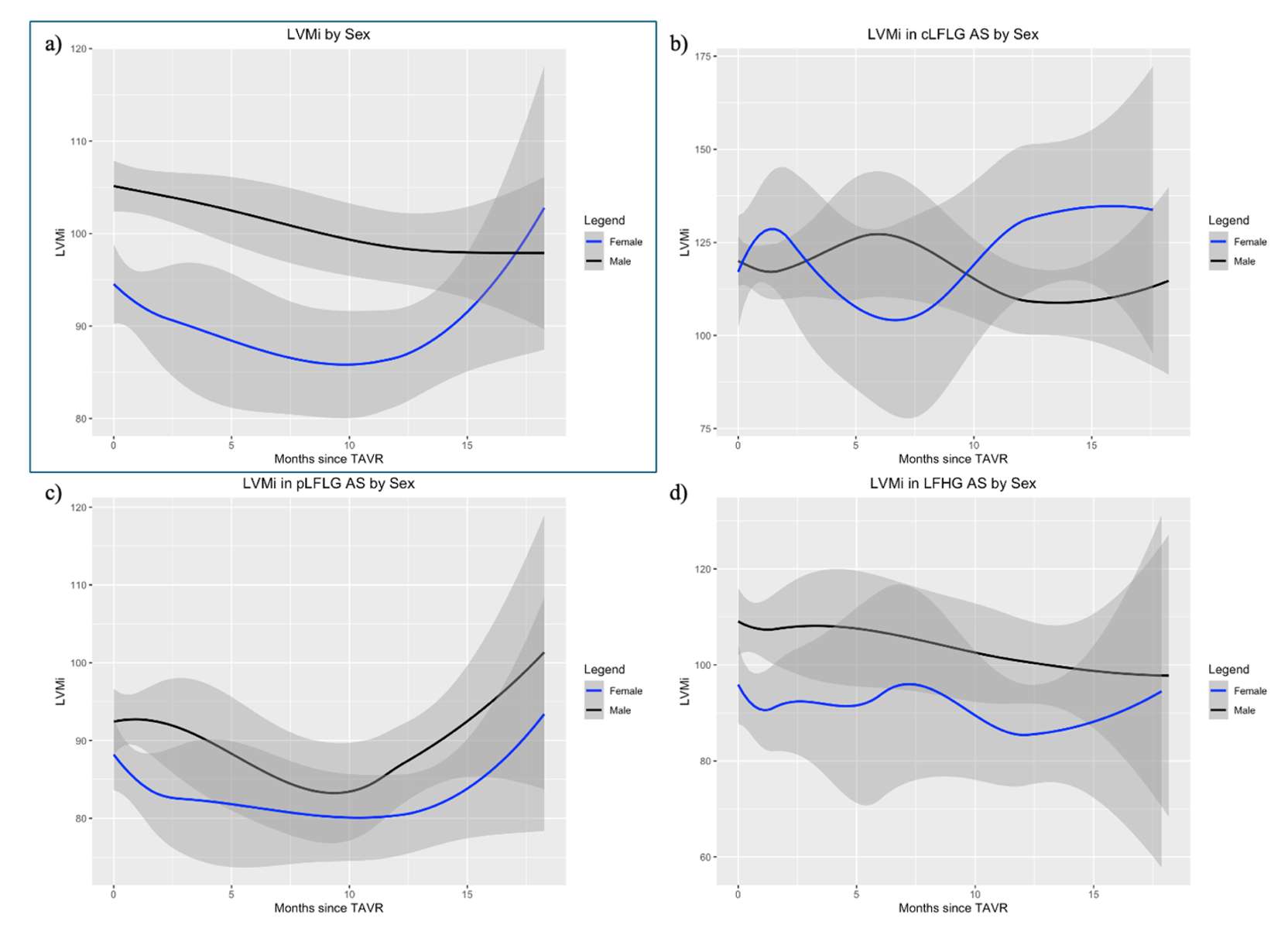
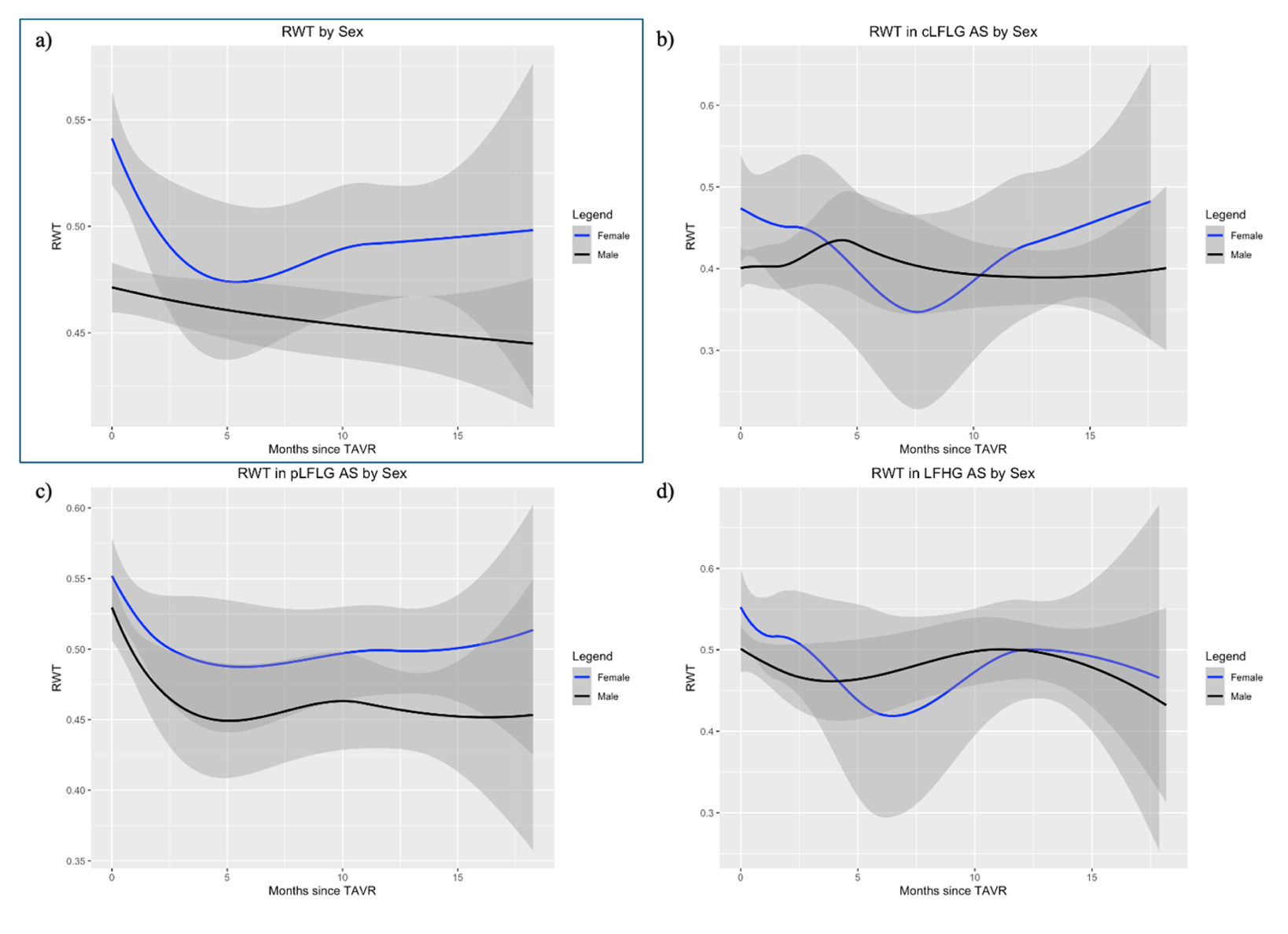
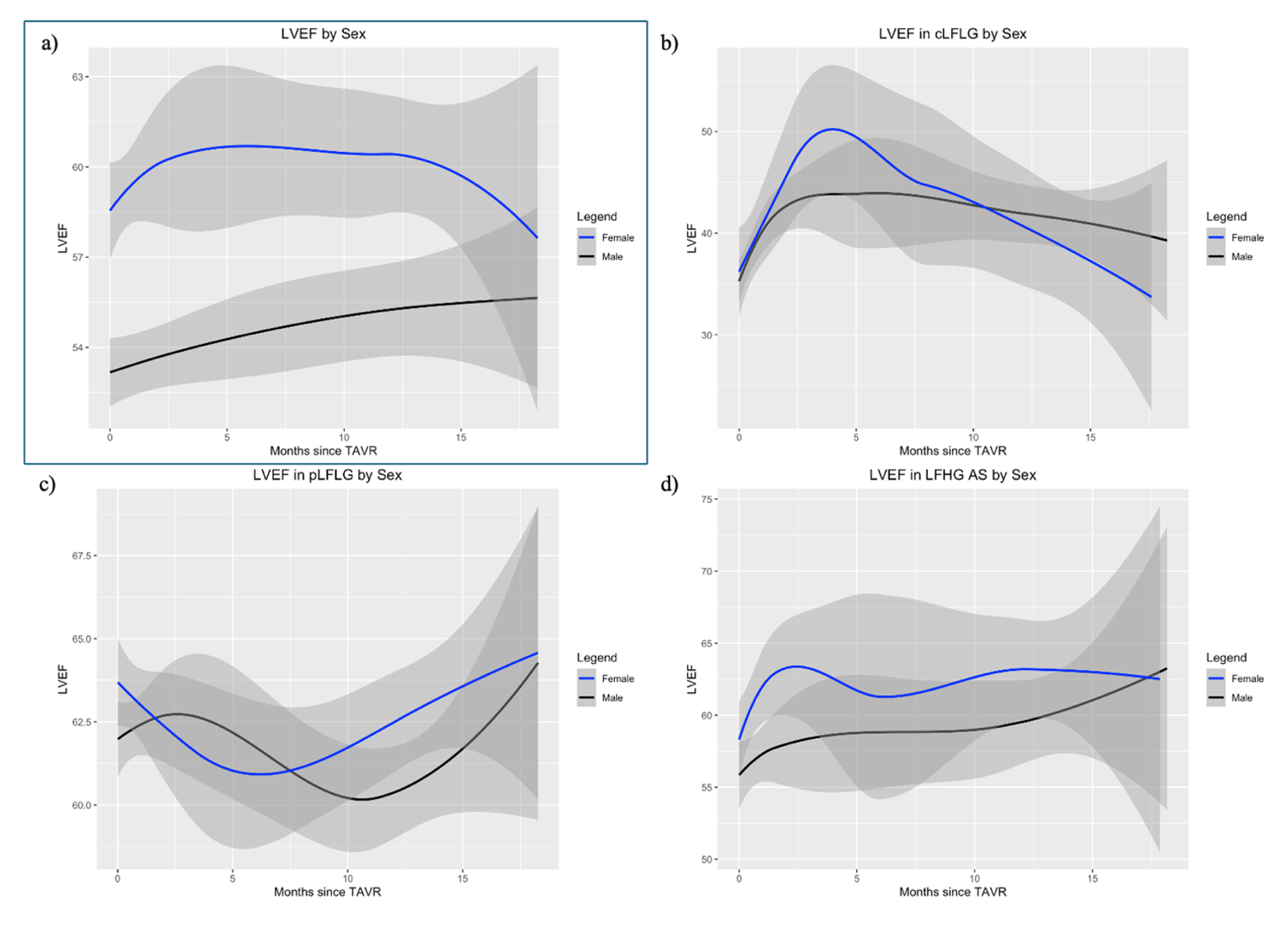
The longitudinal trajectories of LVMi, RWT, and LVEF up to 18 months post-TAVR are presented in Figures 2, 3, and 4.
LVMi decreased progressively during the first year post-TAVR in both sexes; however, after this period, men continued to show a gradual decline, whereas women exhibited stabilization or slight increase (Figure 2A). In the cLFLG group, a sinusoidal pattern of LVMi evolution was observed in both sexes (Figure 2B). In the pLFLG subgroup, both sexes demonstrated an initial reduction in LVMi followed by an increase (Figure 2C), while LVMi slowly declined in the LFHG subgroup (Figure 2D).
RWT declined over time in both sexes (Figure 3A). In men, the decrease was gradual throughout the follow-up period; in women, a steeper initial reduction was observed during the early months, followed by stabilization. Changes in RWT were more pronounced in the pLFLG group compared with the cLFLG and LFHG subgroups, with similar trends in both sexes (Figure 3B-D).
LVEF increased steadily in men; conversely, women exhibited an initial increase up to 3 months post-TAVR, followed by a plateau and subsequent decline approaching 12 months (Figure 4A). This pattern was most evident in the cLFLG subgroup, where women showed a sharper initial rise and steeper decline in LVEF compared with men (Figure 4B). Conversely, in the pLFLG subgroup, LVEF initially decreased in women and subsequently improved around 5 months; in men, there were more fluctuations with inflection points at 3 months and 10 months (Figure 4C).
Changes in echocardiographic parameters according to sex and subtype at 1 year post-TAVR
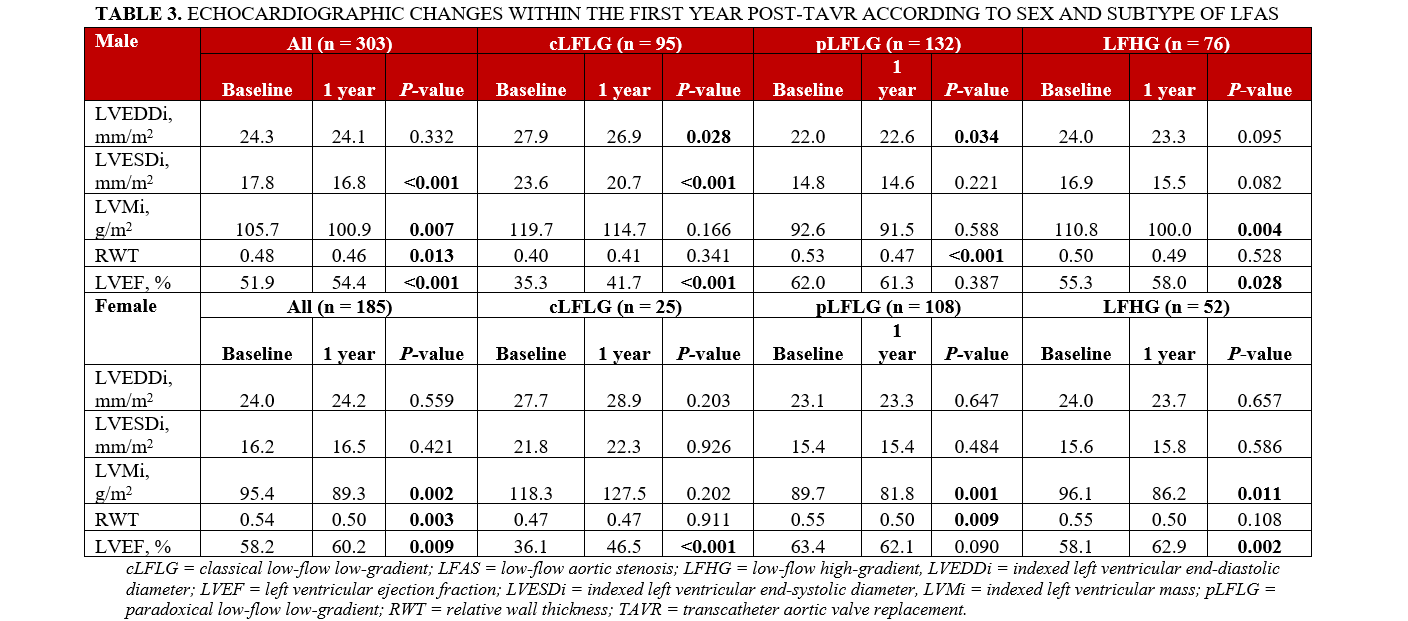
At 1 year post-TAVR, there were statistically significant changes in LVMi, RWT, and LVEF in both male and female cohorts (P < .020 for all) (Table 3). In both groups, there was a decrease in LVMi (105.7-100.9 g/m2 in men, P = .007; 95.4-89.3 g/m2 in women, P = .002) and RWT (0.48-0.46 in men, P = .013; 0.54-0.50 in women, P = .003), while LVEF increased (51.9%-54.4% in men, P < .001; 58.2%-60.2% in women, P = .009). Upon further examination by LFAS subtype, it appeared that, in both sexes, changes in RWT were driven by the pLFLG subgroup, while changes in LVEF were driven by the cLFLG and LFHG subgroups. LVMi significantly decreased in the LFHG subgroup for both sexes; the pLFLG subgroup also saw a significant decline in LVMi for women, but not for men.
Factors associated with LV changes after TAVR
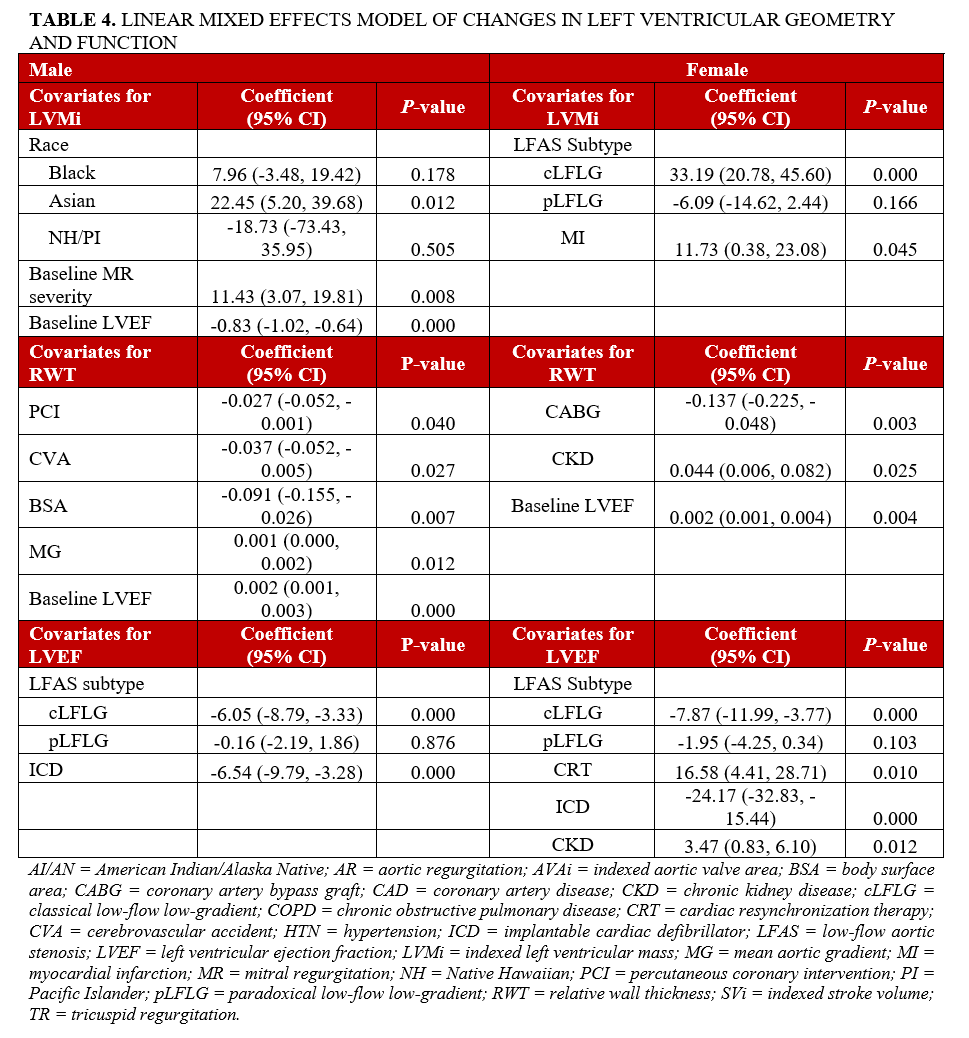
A linear mixed model of post-TAVR changes are summarized in Table 4. In men, more severe baseline MR, lower baseline LVEF, and Asian race were associated with increases in LVMi at follow-up. In women, the cLFLG subtype and prior history of myocardial infarction were associated with an LVMi increase. In men, reductions in RWT were associated with prior history of percutaneous coronary intervention, cerebrovascular accident, higher body surface area, lower MG, and lower baseline LVEF. In women, history of coronary artery bypass grafting, lower baseline LVEF, and no prior history of chronic kidney disease (CKD) were associated with decrease in RWT. Finally, the cLFLG subtype and prior implantable cardiac defibrillator were associated with declines in LVEF in both sexes. In women, cardiac resynchronization therapy and prior CKD were also associated with increase in LVEF.
Notably, a significant interaction was observed between sex and the cLFLG subtype on LVMi (β = −22.35 g/m², P = .003). In females, cLFLG was associated with greater increases in LVMi compared with LFHG (β = 35.26 g/m², P < .001). In males, this difference was attenuated (net effect = 35.26 – 22.35 = 12.91 g/m²). No significant interactions between sex and LFAS subtype were observed for changes in RWT or LVEF.
Discussion
The main findings of this study are (1) both men and women with LFAS demonstrated significant cardiac remodeling after TAVR, with reductions in LVMi and RWT and improvement in LVEF at 1 year, confirming the expected reverse remodeling response to afterload relief in this high-risk population; (2) the longitudinal trajectories of LV remodeling were sex-specific, with men exhibiting gradual, sustained improvement in all parameters throughout the 18-month follow-up and women showing earlier but less sustained changes, specifically a plateau and subsequent partial decline in LVEF after approximately 12 months; and (3) predictors of post-TAVR cardiac remodeling differed significantly between sexes—LFAS subtype was the dominant predictor of LVMi change in women, with the pLFLG subtype associated with favorable regression, while concurrent MR severity and race were the primary determinants in men.
Sex-specific differences in baseline characteristics and LF AS subtypes
The baseline differences between sexes align with established patterns in AS. In our study, men presented with higher rates of comorbidities, consistent with their generally higher cardiovascular risk profile. Conversely, women had higher STS scores, lower LVMi, and greater RWT, reflecting higher degree of concentric remodeling. This is consistent with the well-documented phenomenon of women presenting later in the disease course because of more adaptive remodeling compared with men.11
It is important to consider that these comorbidities are linked with progression to different subtypes of LFAS. The predominance of pLFLG AS in women (58.4% vs 43.6% in men) and cLFLG AS in men (31.4% vs 13.5% in women) may reflect a combination of different comorbidity profiles and fundamental differences in the pathophysiology of AS progression. In our cohort, men had significantly higher rates of CAD and prior coronary interventions, comorbidities that are linked to systolic dysfunction and development of cLFLG AS. Women's tendency toward pLFLG AS likely reflects preserved LVEF despite severe stenosis, possibly due to smaller cavity size, concentric remodeling patterns, and diffuse fibrosis that maintain systolic function at the expense of diastolic filling.12 This finding has important therapeutic implications, as prior literature suggests these subtypes can respond differently to valve replacement. Specifically, pLFLG AS and small LV size are both associated with poor outcomes.13,14
Interestingly, women were more likely to undergo TAVR with SEV, while most men received BEV. This difference has been previously reported15 and could be attributed to SEV providing the more suitable option for smaller annular size in women.
Immediate postprocedural changes
Although too early to assess for reverse remodeling, postprocedural echocardiogram obtained within 24 hours of TAVR can reveal early valvular hemodynamic responses that can lead to long-term changes. In our cohort, women had significantly greater post-TAVR SVi compared with men and were less likely to have mild and/or moderate patient-prosthesis mismatch (PPM). These swift changes may allow for the more rapid improvements in LV geometry seen in women during the early post-TAVR period described below.
Longitudinal patterns of LV remodeling
While LV remodeling showed similar directional changes in both sexes, the trajectories differed markedly: men exhibited gradual, sustained changes, whereas women showed initial rapid changes followed by eventual stabilization. Analysis by LFAS subtype revealed similar patterns within each subtype. Combined with significant baseline differences in subtype distribution between sexes, this suggests that a key component of sex differences in remodeling may be greater proclivity toward pLFLG in women, while men showed a more even distribution across subtypes.
The progressive reduction in LVMi during the first year post-TAVR demonstrates the expected reverse remodeling response to afterload reduction. However, the sex-specific divergence beyond 12 months is striking. While men continued gradual LVMi reduction, women showed stabilization or slight increases, suggesting different adaptive responses to the hemodynamic changes. This pattern may reflect women's baseline tendency toward concentric hypertrophy, which may be more resistant to regression, or differences in neurohormonal responses to afterload relief.12
The subtype-specific patterns further illuminate these mechanisms. The sinusoidal pattern observed in cLFLG patients suggests a more complex remodeling process in patients with severely impaired baseline function, potentially reflecting the interplay between myocardial recovery and ongoing pathophysiologic processes.
The more pronounced initial reduction in RWT in women, followed by stabilization, contrasts with the gradual, sustained decline in men. This pattern suggests that women may achieve optimal wall thickness geometry more rapidly and then maintain this configuration, while men undergo more prolonged geometric remodeling. The predominant changes in the pLFLG subgroup align with this phenotype's baseline concentric remodeling pattern, where wall thickness normalization would be most apparent.
In terms of LV function, men demonstrated sustained improvement throughout follow-up, consistent with expected recovery from afterload reduction. In contrast, women's biphasic pattern—initial improvement followed by decline—warrants careful consideration. This pattern was most pronounced in cLFLG patients, suggesting that women with impaired baseline function may experience incomplete or transient recovery.
Several mechanisms could explain this finding. Women may have greater baseline diastolic dysfunction that limits sustained functional improvement, or, sex-specific differences in myocardial fibrosis and cellular remodeling capacity may influence recovery trajectories.16 The initial improvement likely reflects acute hemodynamic benefits, while the subsequent decline may represent unveiling of underlying myocardial pathology previously masked by severe afterload.17,18
Clinical implications of sex-specific predictors
In men, the association between baseline MR and increased LVMi suggests that addressing concurrent valvular disease may optimize remodeling outcomes. The racial associations observed require further investigation but may reflect genetic or environmental factors influencing cardiac remodeling capacity. In women, the strong association between LFAS subtype and remodeling patterns reinforces the importance of accurate phenotyping. The opposing effects of cLFLG (associated with LVMi increases) and pLFLG (associated with decreases) subtypes suggest fundamentally different pathophysiologic processes that may benefit from tailored therapeutic approaches.
Limitations
Several limitations should be acknowledged. The observational design limits causal inferences, and the relatively modest sample size may have limited power to detect smaller effect sizes, particularly in subgroup analyses. The 18-month follow-up period, while substantial, may not capture long-term remodeling patterns that could differ between sexes. Only a subset of patients (31.7%) underwent dobutamine stress test to confirm LFLG AS. Finally, inter-reader variability may impact echocardiographic assessment.
Conclusions
This study demonstrates that cardiac remodeling following TAVR in patients with LFAS is substantial but heterogeneous, with distinct patterns observed according to sex and LFAS subtype. Reductions in LVMi and RWT, as well as improvements in LVEF, were observed in both sexes at 1 year; however, men exhibited more sustained remodeling trajectories over 18 months, while women showed earlier changes that were less durable, particularly with respect to LVEF. Predictors of remodeling were sex-specific, with LFAS subtype driving structural changes in women and comorbid valvular burden in men.
Affiliations and Disclosures
Eileen Galvani, MD1; Oludamilola Akinmolayemi, MD, MPH2; Philippe Pibarot, DVM, PhD3; Sébastien Hecht, PhD3; Roya Anahita Mousavi, MD2; Yash Prakash, MD1; Esha Vaish, MD1; Samin K. Sharma, MD2; Annapoorna Kini, MD2; Marie-Annick Clavel, DVM, PhD3; Stamatios Lerakis, MD, PhD2
From the 1Department of Medicine, Mount Sinai Hospital, Icahn School of Medicine at Mount Sinai, New York, New York; 2Department of Cardiology, Mount Sinai Fuster Heart Hospital, Icahn School of Medicine at Mount Sinai, New York, New York; 3Institut Universitaire de Cardiologie et de Pneumologie de Québec/Québec Heart and Lung Institute, Department of Medicine, Laval University, Québec City, Québec, Canada.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Stamatios Lerakis, MD, PhD, Mount Sinai Fuster Heart Hospital, 1 Gustave L. Levy Pl, Box 1030, New York, NY 10029, USA. Email: stamatios.lerakis@mountsinai.org
References
1. Praz F, Borger MA, Lanz J, et al; ESC/EACTS Scientific Document Group. 2025 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2025;46(44):4635-4736. doi:10.1093/eurheartj/ehaf194
2. Isselbacher EM, Preventza O, Hamilton Black J III, et al; Peer Review Committee Members. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology joint committee on clinical practice guidelines. Circulation. 2022;146(24):e334-e482. doi:10.1161/CIR.0000000000001106
3. Treibel TA, Badiani S, Lloyd G, Moon JC. Multimodality imaging markers of adverse myocardial remodeling in aortic stenosis. JACC Cardiovasc Imaging. 2019;12(8 Pt 1):1532-1548. doi:10.1016/j.jcmg.2019.02.034
4. Heydari B, Jerosch-Herold M. Left ventricular remodeling in aortic stenosis and systemic hypertension: phenotypical look-alikes or distinct siblings? Circ Cardiovasc Imaging. 2024;17(8):e017266. doi:10.1161/CIRCIMAGING.124.017266
5. Kuneman JH, Butcher SC, Stassen J, et al. Interaction between sex and left ventricular reverse remodeling and its association with outcomes after transcatheter aortic valve implantation. Int J Cardiovasc Imaging. 2022;38(9):1973-1985. doi:10.1007/s10554-022-02596-x
6. Ninomiya R, Orii M, Fujiwara J, et al. Sex-related differences in cardiac remodeling and reverse remodeling after transcatheter aortic valve implantation in patients with severe aortic stenosis in a Japanese population. Int Heart J. 2020;61(5):961-969. doi:10.1536/ihj.20-154
7. Chen SC, Leu HB, Chang HH, et al. Women had favourable reverse left ventricle remodelling after TAVR. Eur J Clin Invest. 2020;50(1):e13183. doi:10.1111/eci.13183
8. Osman M, Ghaffar YA, Foster T, et al. Meta-analysis of outcomes of transcatheter aortic valve implantation among patients with low gradient severe aortic stenosis. Am J Cardiol. 2019;124(3):423-429. doi:10.1016/j.amjcard.2019.05.006
9. Wagener M, Reuthebuch O, Heg D, et al. Clinical outcomes in high-gradient, classical low-flow, low-gradient, and paradoxical low-flow, low-gradient aortic stenosis after transcatheter aortic valve implantation: a report from the SwissTAVI Registry. J Am Heart Assoc. 2023;12(12):e029489. doi:10.1161/JAHA.123.029489
10. Mitchell C, Rahko PS, Blauwet LA, et al. Guidelines for performing a comprehensive transthoracic echocardiographic examination in adults: recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr. 2019;32(1):1-64. doi:10.1016/j.echo.2018.06.004
11. Tribouilloy C, Bohbot Y, Rusinaru D, et al. Excess mortality and undertreatment of women with severe aortic stenosis. J Am Heart Assoc. 2021;10(1):e018816. doi:10.1161/JAHA.120.018816
12. Aggarwal A, Kumar M, Abid S, Khlidj Y, Davila CD. Gender disparity in the treatment of aortic stenosis. Curr Treat Options Cardio Med. 2025;27(1):1-10. doi:10.1007/s11936-025-01108-z
13. Saito T, Inohara T, Yoshijima N, et al. Small left ventricle and clinical outcomes after transcatheter aortic valve replacement. J Am Heart Assoc. 2021;10(7):e019543. doi:10.1161/JAHA.120.019543
14. Springhetti P, Abdoun K, Clavel MA. Sex differences in aortic stenosis: from the pathophysiology to the intervention, current challenges, and future perspectives. J Clin Med. 2024;13(14):4237. doi:10.3390/jcm13144237
15. Tateishi K, Hmoud H, De Gregorio I, Hastings R, De Gregorio J. The impact of gender on outcomes of transcatheter aortic valve implantation between self-expanding valve and balloon-expandable valve. Cardiovasc Revasc Med. 2024;63:38-42. doi:10.1016/j.carrev.2024.01.002
16. Iribarren AC, AlBadri A, Wei J, et al. Sex differences in aortic stenosis: Identification of knowledge gaps for sex-specific personalized medicine. Am Heart J Plus. 2022;21:100197. doi:10.1016/j.ahjo.2022.100197
17. Le Nezet E, Marqueze-Pouey C, Guisle I, Clavel MA. Molecular features of calcific aortic stenosis in female and male patients. CJC Open. 2024;6(9):1125-1137. doi:10.1016/j.cjco.2024.06.002
18. Voisine M, Hervault M, Shen M, et al. Age, sex, and valve phenotype differences in fibro-calcific remodeling of calcified aortic valve. J Am Heart Assoc. 2020;9(10):e015610. doi:10.1161/JAHA.119.015610












