


Coronary Computed Tomography Angiography to Guide Percutaneous Coronary Intervention: Proceedings From the 1st CCTA-Guided PCI Summit in the United States
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00085. Epub June 23, 2026.
Abstract
Coronary computed tomography angiography (CCTA) can be used beyond diagnostic purposes to support the preprocedural planning of percutaneous coronary intervention (PCI). Advances in scanner technology, software platforms, and physiology- and plaque-based visualization tools have expanded the role of CCTA-guided PCI. CCTA provides detailed assessment of coronary anatomy, plaque and calcium morphology, lesion length, vessel size, and noninvasive physiology, offering opportunities to anticipate procedural complexity, optimize resource utilization, and individualize PCI strategy. Emerging data, including randomized studies in chronic total occlusions and ongoing multicenter trials, support the feasibility and potential clinical value of this approach. In April 2024, the first CCTA-guided PCI summit in the United States convened interventional cardiologists and cardiac imagers, as well as industry stakeholders, to discuss the evidence, technical considerations, clinical applications, and unmet needs related to CCTA-guided PCI. This manuscript summarizes the key discussions and conclusions specific to this meeting, with a focus on the transition of CCTA from a diagnostic to a therapeutic planning tool, emerging artificial intelligence applications, its complementary role with intravascular imaging, and opportunities to enhance procedural planning and decision-making. While early experience is promising, broader adoption will require broader educational efforts, access to purpose-built visualization software tools designed for interventional cardiologists, multidisciplinary collaboration, and additional randomized and real-world studies to define its impact on clinical outcomes and procedural efficiency.
Introduction
Coronary computed tomography angiography (CCTA) is increasingly used to guide percutaneous coronary intervention (PCI). It can be used for preprocedural planning, as well as for intraprocedural guidance with C-arm and CCTA co-registration. The emerging opportunities with CCTA-guided PCI are enabled by several converging factors, including improvements in scanner technology, the development of scalable software solutions, the use of artificial intelligence (AI), greater technical expertise in image acquisition and interpretation, multidisciplinary collaboration, and increased availability and ease of access to CCTA. Additional drivers include the translation of lessons learned from transcatheter structural interventions and the heart-team approach, the increasing use of CCTA in patients with suspected or established acute or chronic coronary syndromes, and growing evidence supporting its use for PCI guidance.
In patients undergoing PCI, intravascular imaging (IVI) and invasive coronary physiology are guideline-recommended tools to inform procedural decision-making based on the assessment of lesion morphology, including plaque characterization and calcium assessment, lesion length, proximal and distal reference vessel diameters, and functional significance. While similar information can be obtained noninvasively from CCTA for preprocedural planning, such data have traditionally not been used in the cardiac catheterization laboratory by interventional cardiologists (IC). This is in part due to limited training and familiarity with the use and interpretation of CCTA, limited access to purpose-built software applications designed for ICs, a paucity of supporting data and lack of established workflows, and limited collaboration with cardiac imagers and radiologists.
In recent years, there have been multiple technical innovations and a growing evidence base to support CCTA-guided PCI. Randomized data support its use to improve PCI success in patients with chronic total occlusions (CTO). There is also an ongoing pivotal P4 (Precise Procedural and PCI Plan) randomized clinical trial evaluating CCTA-guided PCI; it compares a structured preprocedural CCTA planning package and intraprocedural guidance with C-arm co-registration with intravascular ultrasound (IVUS), with 1-year major adverse cardiovascular events (MACE) as the primary endpoint, further accelerating interest in this space. While educational efforts have taken place in Europe, there is limited awareness and understanding about the potential opportunities with CCTA in the United States.
To educate and discuss opportunities with CCTA-guided PCI, we organized the first US-based CCTA-guided PCI summit.
THE FIRST US CCTA-GUIDED PCI SUMMIT
During a 1.5-day meeting held from April 4 to 5, 2024, in Minneapolis, Minnesota, stakeholders from academia, ICs, and cardiac imagers (including noninvasive cardiologists and radiologists), as well as industry, considered the challenges and opportunities of CCTA-guided PCI. This meeting was organized by Drs Yader Sandoval, João L. Cavalcante, and Emmanouil S. Brilakis through the Center for Coronary Artery Disease at the Minneapolis Heart Institute Foundation (MHIF) in partnership with the Allina Health Minneapolis Heart Institute. The meeting included 76 participants, primarily from from the United States, along with key opinion leaders from Europe and Canada. Physicians with expertise in interventional cardiology, including coronary physiology, IVI, complex coronary interventions, and/or CCTA imaging were recruited through direct invitation by the meeting organizers.
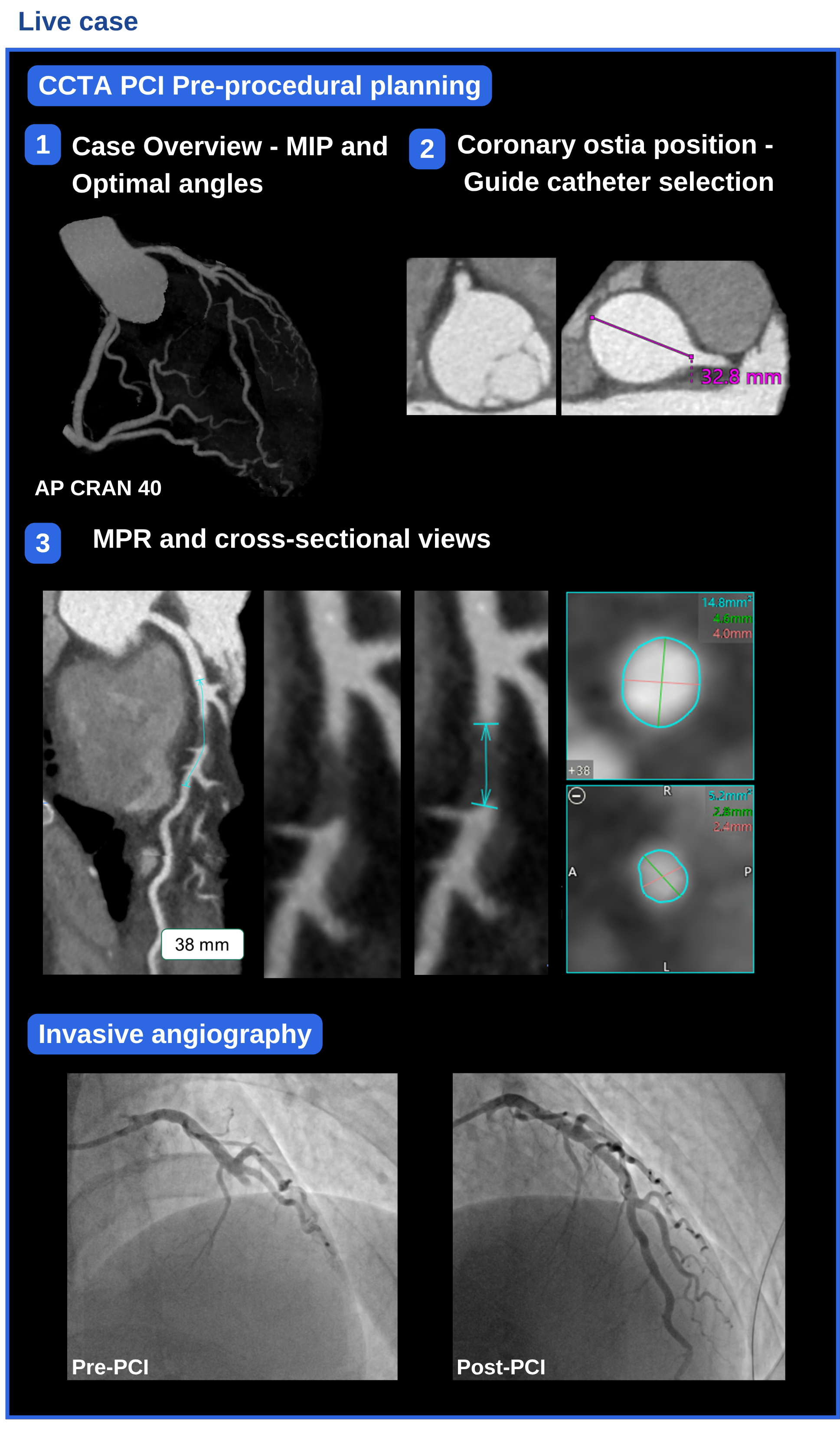
The meeting format consisted of alternating sessions of brief moderated presentations following a formal agenda and faculty-led discussions. Additionally, the meeting included hands-on training sessions, and live CCTA-guided PCI cases (Figure 1). Detailed notes were recorded during the meeting describing the presentations and discussion. The statements in this manuscript were not derived through a voting process; rather, the manuscript was circulated among the faculty, who reviewed and refined the key messages from this scientific summit. Presenters shared their slide sets for reference during the manuscript development. This paper summarizes the discussion and conclusions of this meeting.
1. CCTA: The transition from a diagnostic to an interventional planning tool
The utilization of CCTA has seen a significant rise in recent years owing to its diagnostic accuracy in identifying coronary artery disease (CAD).
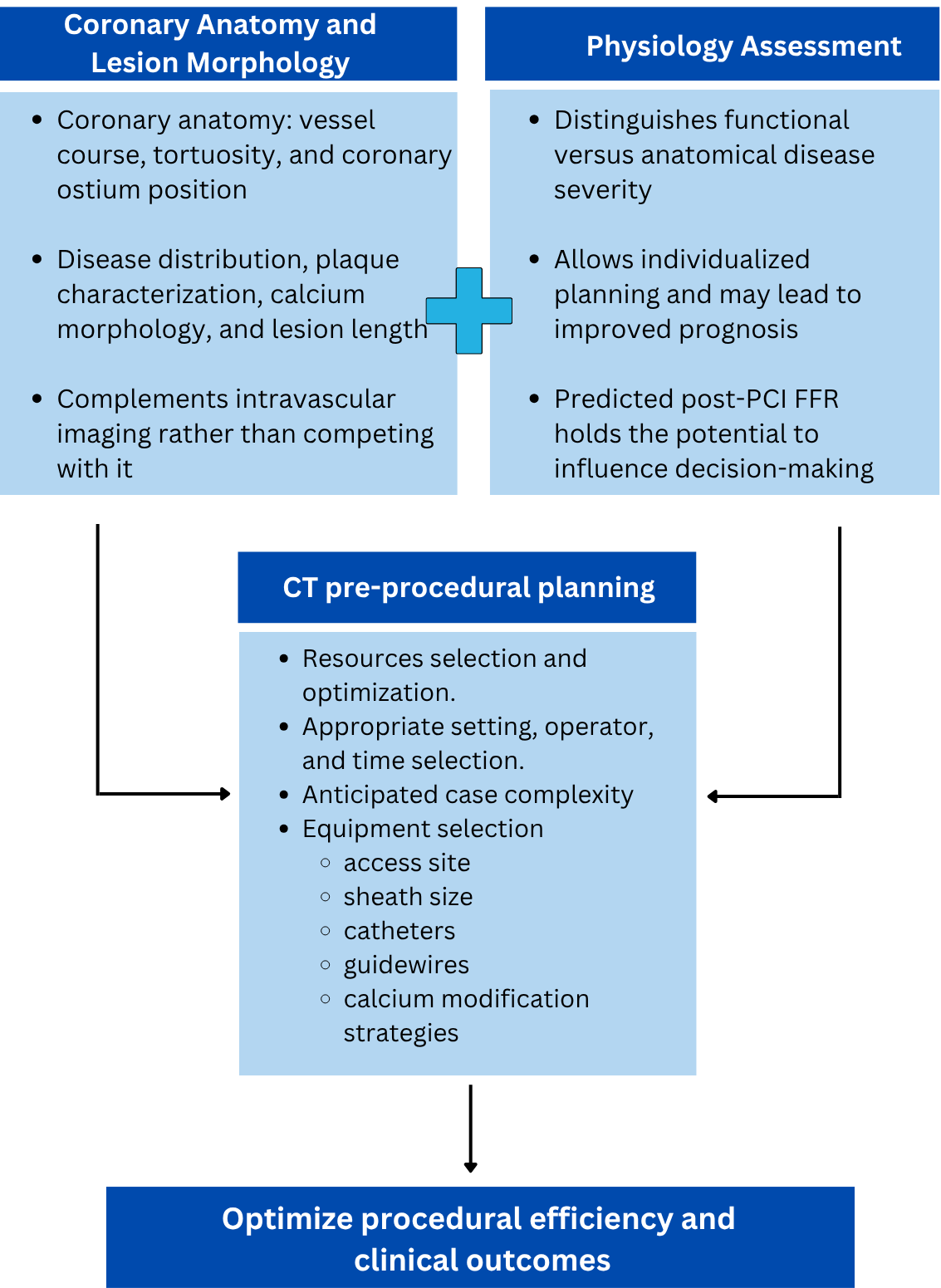
Moving beyond diagnosis, in patients suitable for PCI, CCTA can provide a comprehensive anatomical and physiological assessment that can aid in preprocedural planning. It enables the optimization of resources based on case complexity and can inform case triage to the appropriate setting (hospital with on-site surgery, hospital without surgery on-site, or ambulatory surgical center), operator, and scheduling. Randomized trials in selected populations, such as patients with CTOs and those with prior coronary artery bypass grafting (CABG), have demonstrated improved procedural efficiency with CCTA-guided PCI.
2. CCTA to analyze lesion morphology, including plaque characterization and calcium assessment, lesion length, and vessel diameter
IVI, utilizing either IVUS or optical coherence tomography (OCT), is used to characterize plaque burden, lesion morphology, and guide stent size and expansion.
CCTA provides preprocedural insights about vessel course and tortuosity, coronary ostium position, and ideal fluoroscopic angles for PCI.
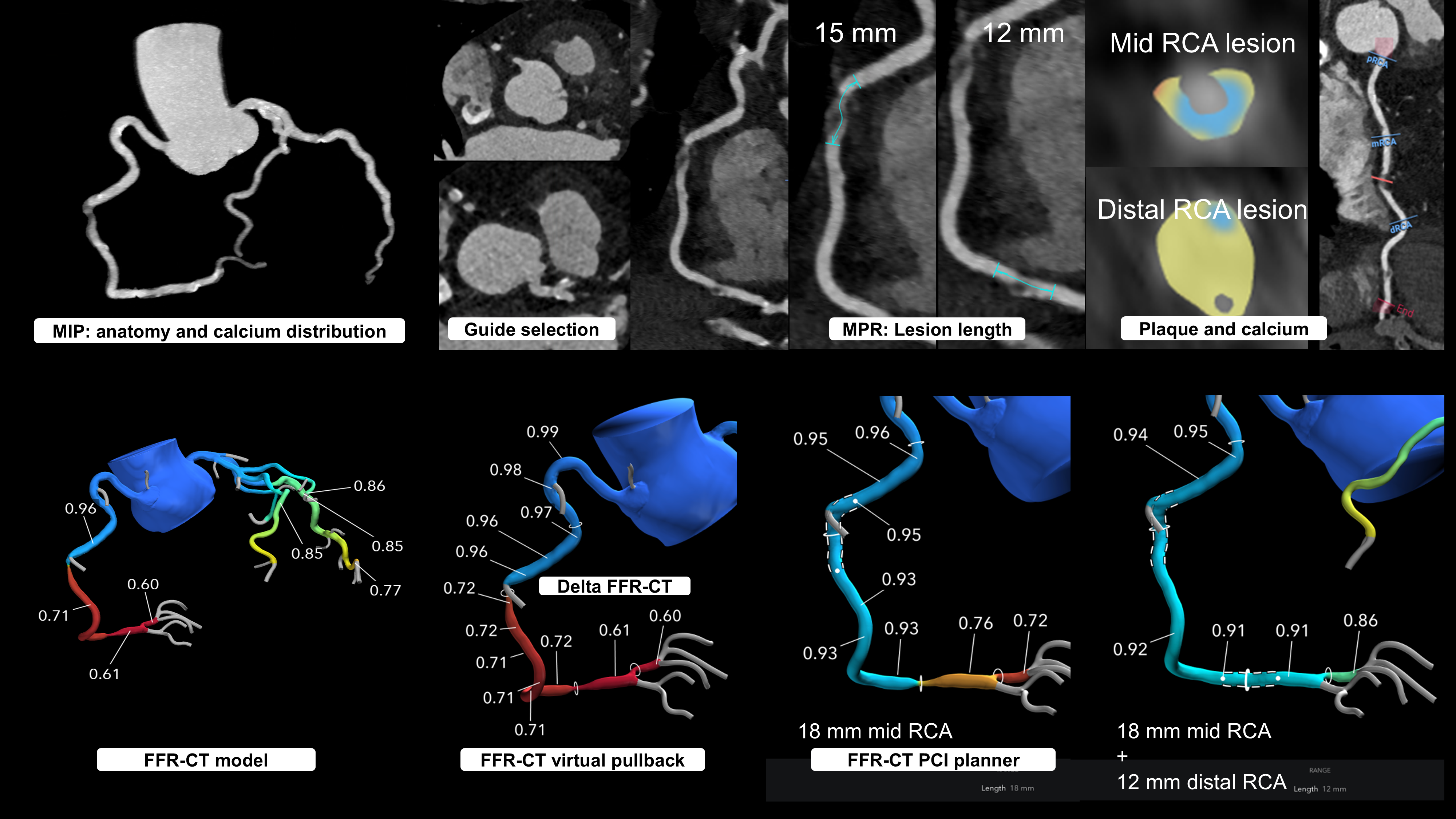
Analogous to IVI, CCTA offers adequate assessments of plaque and calcium morphology, as well as lesion length, to inform PCI planning. While traditional energy-integrated CCTA overestimates calcium volume, correlation studies with OCT indicate that calcium arc and length can be assessed adequately with CCTA and potentially inform the need for calcium modification strategies.
Opportunities remain to standardize vessel diameter assessment using CCTA. With IVI, when visible, the external elastic lamina (EEL) is the preferred approach to guide stent sizing (down-sizing stent size based on cross-sectional EEL measurements) or lumen-based assessments (and upsizing stent size) when the EEL is not well visualized.
Ongoing registry studies like the INVICTUS (Multicenter Registry of Invasive and Non-Invasive imaging modalities to compare Coronary Computed Tomography Angiography, Intravascular Ultrasound and Optical Coherence Tomography for the determination of Severity, Volume and Type of coronary atherosclerosis) registry aim to elucidate the agreement between CCTA and IVI in measuring the stent size and disease severity.
Challenges also persist in differentiating between fibrous and fibro-fatty plaques due to similar Hounsfield units between these 2 types of plaques.
3. CCTA physiology and virtual PCI
A key advantage of CCTA is the integration of anatomical and physiological data to guide invasive angiography and PCI. FFRCT demonstrates diagnostic performance comparable to invasive pressure wire assessment and superior to perfusion imaging.
The CCTA virtual planner allows the performance of virtual PCI, offering benefits such as equipment selection, stent sizing, optimization of visualization angles, and pre- and virtually predicted post-procedural physiology. Predicted post-PCI FFRCT has been validated against pressure-wire post-PCI FFR as well as angiographic post-PCI FFR.
In addition, CCTA can also assess the myocardial mass subtended, which is particularly relevant for bifurcation procedures, aiding in decision-making regarding side branch wire protection or stenting.
4. Clinical applications and unmet needs
CCTA plays a crucial role beyond diagnosis by providing guidance and enhancing preparedness for PCI procedures in the catheterization laboratory. CCTA integration facilitates optimized resource allocation, improved procedural outcomes, and shared decision-making between clinicians and patients. To date, randomized controlled trials (RCTs) have shown increased procedural efficiency with CCTA-guided PCI in patients with CTO and prior CABG. The clinical benefit of CCTA‑guided PCI is being evaluated in the ongoing P4 trial, while additional RCTs are warranted to better define patient and lesion subsets most likely to benefit.
Although CCTA exhibits some limitations in lesion assessment and characterization, these challenges can be addressed through integration with complementary imaging modalities.
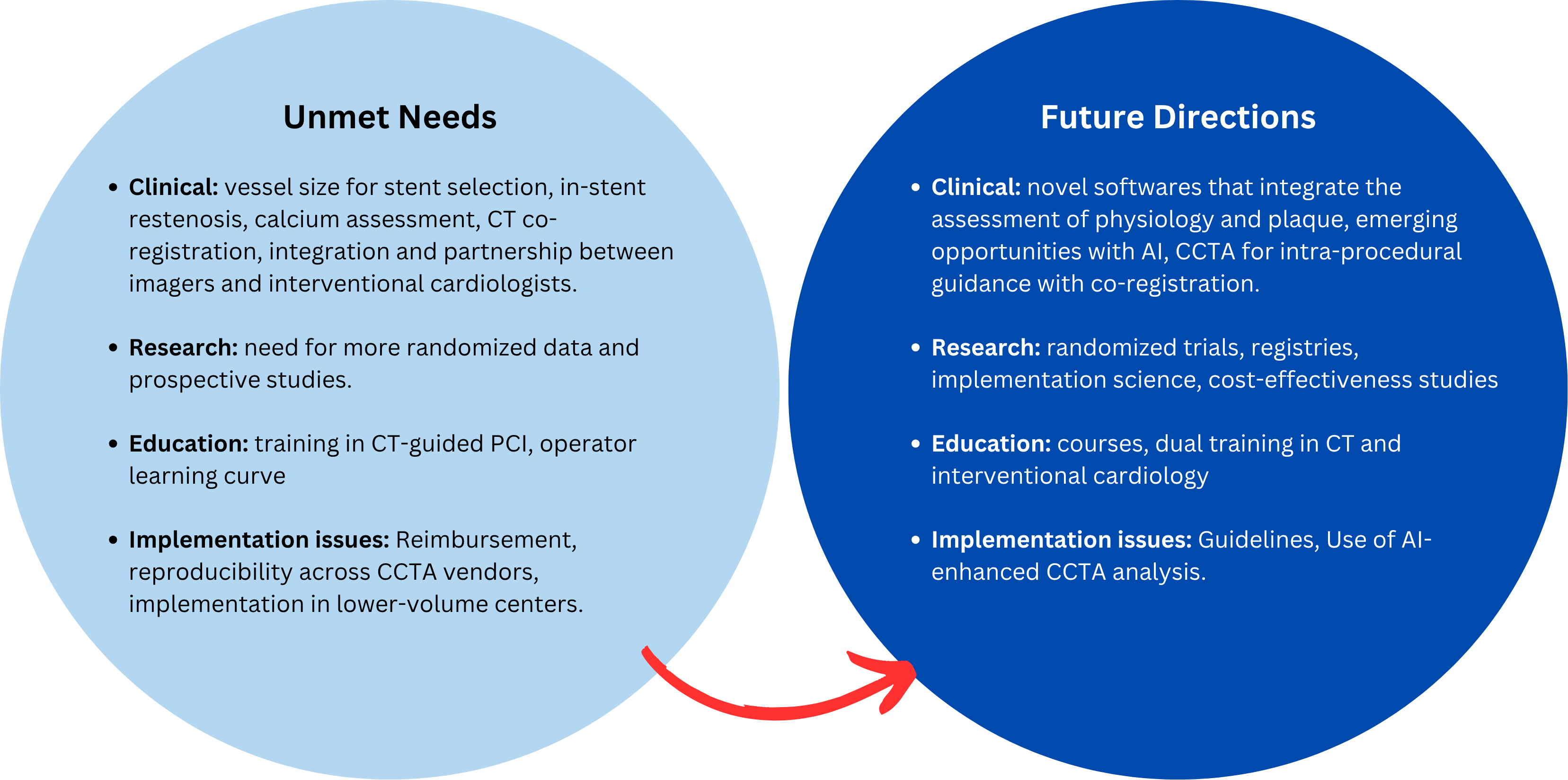
The disparity in spatial-temporal resolution between CCTA and invasive intracoronary imaging underscores the challenges faced. Nonetheless, current discussions and available evidence do not sufficiently address practical barriers to real‑world implementation of CCTA-guided PCI, including scan‑to‑procedure time, reproducibility across CCTA vendors and software platforms, reimbursement considerations, data integration into the catheterization laboratory workflow, operator learning curves with CCTA interpretation, and the feasibility of adopting CCTA‑guided PCI in lower‑volume centers. Advancements in new AI-based tools may facilitate data extraction, accelerate the learning curve, and improve agreement between imaging modalities and physicians (Figure 3). Also, the co-registration of multiple techniques during PCI procedures offers synergistic benefits.
Conclusions
CCTA has evolved from a diagnostic modality to an important tool for preprocedural planning and PCI guidance. Broader adoption will require broader educational efforts, access to purpose-built software designed for ICs, and close collaboration with cardiac imaging physicians. While early data are promising, additional randomized and real-world studies are needed to define its impact on clinical outcomes and procedural efficiency.
Affiliations and Disclosures
Pedro E.P. Carvalho, MD1; João L. Cavalcante, MD1,2; Carlos Collet, MD, PhD3; Jonathon Leipsic, MD4; Omar K. Khalique, MD5; Victor Cheng, MD2; John Lesser, MD2; Bavana Rangan, BDS, MPH2; Emmanouil S. Brilakis, MD, PhD1,2; Yader Sandoval, MD1,2
From the 1Center for Coronary Artery Disease, Minneapolis Heart Institute Foundation, Minneapolis, Minnesota; 2Minneapolis Heart Institute, Abbott Northwestern Hospital, Minneapolis, Minnesota; 3Cardiovascular Center Aalst, OLV Clinic, Aalst, Belgium; 4Department of Medicine and Radiology, University of British Columbia, Vancouver, British Columbia, Canada; 5St Francis Hospital and Heart Center, Roslyn, New York.
Acknowledgments: The authors would like to thank the Center for Coronary Artery Disease for its support in the first CCTA‑guided PCI initiative, with particular appreciation to Dimitris Strepkos, Michaella Alexandrou, Olga Mastrodemos, Deniz Mutlu, and Athanasios Rempakos.
Disclosures: Dr Leipsic is a consultant for, and holds stock options in Heartflow. Dr Khalique is a consultant for Heartflow, Siemens, and Philips. Dr Cheng serves as a scientific advisor for Cleerly Health. Dr Brilakis receives consulting/speaker honoraria from Abbott Vascular, the American Heart Association (associate editor, Circulation), Boston Scientific, the Cardiovascular Innovations Foundation (Board of Directors), Cordis, Elsevier, GE Healthcare, Heartflow, IMDS, Medtronic, Recor Medical, Shockwave, SIS Medical, Teleflex, and Terumo; receives research support from AngioWave, Boston Scientific, and GE Healthcare; is the owner of Hippocrates LLC and Systole LLC; and is a shareholder in Cleerly Health, LifeLens Technologies, Inc., MHI Ventures, Stallion Medical, and TrueVue, Inc. Dr Sandoval reports relationships with Abbott Vascular (consultant, advisory board, speaker); Boston Scientific (consultant); CathWorks (consultant, speaker); Cleerly Health (speaker, research grant); GE Healthcare (consultant, advisory board, speaker); HeartFlow (consultant, advisory board, speaker, research grant); Medtronic (speaker); Philips (consultant, advisory board, speaker); Roche Diagnostics (consultant, advisory board, speaker); Siemens (consultant, advisory board); and Shockwave Medical (research/education grant); and jointly holds patent 20210401347. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Yader Sandoval, MD, FACC, FSCAI, FESC, Minneapolis Heart Institute, Abbott Northwestern Hospital and Center for Coronary Artery Disease, Minneapolis Heart Institute Foundation, 920 East 28th Street, Suite 300, Minneapolis, MN 55407, USA. Email: yadersandoval@gmail.com; X: @yadersandoval
References
1. Haase R, Schlattmann P, Gueret P, et al; COME-CCT Consortium. Diagnosis of obstructive coronary artery disease using computed tomography angiography in patients with stable chest pain depending on clinical probability and in clinically important subgroups: meta-analysis of individual patient data. BMJ. 2019;365:l1945. doi:10.1136/bmj.l1945
2. Linde JJ, Kofoed KF, Sørgaard M, et al. Cardiac computed tomography guided treatment strategy in patients with recent acute-onset chest pain: results from the randomised, controlled trial: CArdiac cT in the treatment of acute CHest pain (CATCH). Int J Cardiol. 2013;168(6):5257-5262. doi:10.1016/j.ijcard.2013.08.020
3. Hoffmann U, Truong QA, Schoenfeld DA, et al; ROMICAT-II Investigators. Coronary CT angiography versus standard evaluation in acute chest pain. N Engl J Med. 2012;367(4):299-308. doi:10.1056/NEJMoa1201161
4. Goldstein JA, Gallagher MJ, O'Neill WW, Ross MA, O'Neil BJ, Raff GL. A randomized controlled trial of multi-slice coronary computed tomography for evaluation of acute chest pain. J Am Coll Cardiol. 2007;49(8):863-871. doi:10.1016/j.jacc.2006.08.064
5. Hoffmann U, Ferencik M, Udelson JE, et al; PROMISE Investigators. Prognostic value of noninvasive cardiovascular testing in patients with stable chest pain: insights from the PROMISE trial (Prospective Multicenter Imaging Study for Evaluation of Chest Pain). Circulation. 2017;135(24):2320-2332. doi:10.1161/CIRCULATIONAHA.116.024360
6. Machado MF, Felix N, Melo PHC, et al. Coronary computed tomography angiography versus invasive coronary angiography in stable chest pain: a meta-analysis of randomized controlled trials. Circ Cardiovasc Imaging. 2023;16(11):e015800. doi:10.1161/CIRCIMAGING.123.015800
7. Patel MR, Peterson ED, Dai D, et al. Low diagnostic yield of elective coronary angiography. N Engl J Med. 2010;362(10):886-895. doi:10.1056/NEJMoa0907272
8. Collet C, Sonck J, Leipsic J, et al. Implementing coronary computed tomography angiography in the catheterization laboratory. JACC Cardiovasc Imaging. 2021;14(9):1846-1855. doi:10.1016/j.jcmg.2020.07.048
9. Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 2021;144(22):e368-e454. doi:10.1161/CIR.0000000000001029
10. Jones DA, Beirne AM, Kelham M, et al; BYPASS-CTCA Trial Committees and Investigators. Computed tomography cardiac angiography before invasive coronary angiography in patients with previous bypass surgery: the BYPASS-CTCA trial. Circulation. 2023;148(18):1371-1380. doi:10.1161/CIRCULATIONAHA.123.064465
11. Hong SJ, Kim BK, Cho I, et al; CT-CTO Investigators. Effect of coronary CTA on chronic total occlusion percutaneous coronary intervention: a randomized trial. JACC Cardiovasc Imaging. 2021;14(10):1993-2004. doi:10.1016/j.jcmg.2021.04.013
12. Maehara A, Matsumura M, Ali ZA, Mintz GS, Stone GW. IVUS-guided versus OCT-guided coronary stent implantation: a critical appraisal. JACC Cardiovasc Imaging. 2017;10(12):1487-1503. doi:10.1016/j.jcmg.2017.09.008
13. Stone GW, Christiansen EH, Ali ZA, et al. Intravascular imaging-guided coronary drug-eluting stent implantation: an updated network meta-analysis. Lancet. 2024;403(10429):824-837. doi:10.1016/S0140-6736(23)02454-6
14. Smilowitz NR, Mohananey D, Razzouk L, Weisz G, Slater JN. Impact and trends of intravascular imaging in diagnostic coronary angiography and percutaneous coronary intervention in inpatients in the United States. Catheter Cardiovasc Interv. 2018;92(6):E410-E415. doi:10.1002/ccd.27673
15. Flattery E, Rahim HM, Petrossian G, et al. Competency-based assessment of interventional cardiology fellows' abilities in intracoronary physiology and imaging. Circ Cardiovasc Interv. 2020;13(2):e008760. doi:10.1161/CIRCINTERVENTIONS.119.008760
16. Naidu SS, Coylewright M, Hawkins BM, et al. Hot topics in interventional cardiology: Proceedings from the society for cardiovascular angiography and interventions 2020 think tank. Catheter Cardiovasc Interv. 2020;96(6):1258-1265. doi:10.1002/ccd.29197
17. Monizzi G, Sonck J, Nagumo S, et al. Quantification of calcium burden by coronary CT angiography compared to optical coherence tomography. Int J Cardiovasc Imaging. 2020;36(12):2393-2402. doi:10.1007/s10554-020-01839-z
18. Kurogi K, Ishii M, Nagatomo T, et al. Mean density of computed tomography for predicting rotational atherectomy during percutaneous coronary intervention. J Cardiovasc Comput Tomogr. 2023;17(2):120-129. doi:10.1016/j.jcct.2023.02.002
19. Uzu K, Otake H, Choi G, et al. Lumen boundaries extracted from coronary computed tomography angiography on computed fractional flow reserve (FFRCT): validation with optical coherence tomography. EuroIntervention. 2019;14(15):e1609-e1618. doi:10.4244/EIJ-D-17-01132
20. Collet C, Chevalier B, Cequier A, et al. Diagnostic accuracy of coronary CT angiography for the evaluation of bioresorbable vascular scaffolds. JACC Cardiovasc Imaging. 2018;11(5):722-732. doi:10.1016/j.jcmg.2017.04.013
21. Nakanishi R, Okubo R, Sobue Y, et al. Rationale and design of the INVICTUS registry: (Multicenter Registry of Invasive and Non-Invasive imaging modalities to compare Coronary Computed Tomography Angiography, Intravascular Ultrasound and Optical Coherence Tomography for the determination of Severity, Volume and Type of coronary atherosclerosiS). J Cardiovasc Comput Tomogr. 2023;17(6):401-406. doi:10.1016/j.jcct.2023.08.011
22. Cao JJ, Shen L, Nguyen J, et al. Accuracy and limitation of plaque detection by coronary CTA: a section-to-section comparison with optical coherence tomography. Sci Rep. 2023;13(1):11845. doi:10.1038/s41598-023-38675-9
23. Wertman BM, Cheng VY, Kar S, et al. Characterization of complex coronary artery stenosis morphology by coronary computed tomographic angiography. JACC Cardiovasc Imaging. 2009;2(8):950-958. doi:10.1016/j.jcmg.2008.12.032
24. Motoyama S, Ito H, Sarai M, et al. Plaque characterization by coronary computed tomography angiography and the likelihood of acute coronary events in mid-term follow-up. J Am Coll Cardiol. 2015;66(4):337-346. doi:10.1016/j.jacc.2015.05.069
25. Andreini D, Collet C, Leipsic J, et al. Pre-procedural planning of coronary revascularization by cardiac computed tomography: an expert consensus document of the Society of Cardiovascular Computed Tomography. J Cardiovasc Comput Tomogr. 2022;16(6):558-572. doi:10.1016/j.jcct.2022.08.003
26. Sonck J, Nagumo S, Norgaard BL, et al. Clinical validation of a virtual planner for coronary interventions based on Coronary CT angiography. JACC Cardiovasc Imaging. 2022;15(7):1242-1255. doi:10.1016/j.jcmg.2022.02.003
27. Carvalho PEP, Cavalcante JL, Lesser J, et al. Comparison of predicted post-PCI FFR derived from coronary computed tomography angiography versus observed angiographic FFR: emerging concept of wireless end-to-end physiology-guided PCI. Cardiovasc Revasc Med. 2025:S1553-8389(25)00624-4. doi:10.1016/j.carrev.2025.12.019
28. Lodi Rizzini M, Nagumo S, Gallo D, et al. Mismatch between morphological and functional assessment of the length of coronary artery disease. Int J Cardiol. 2021;334:1-9. doi:10.1016/j.ijcard.2021.04.046
29. Van Belle E, Raposo L, Bravo Baptista S, et al. Impact of an interactive CT/FFRCT interventional planner on coronary artery disease management decision making. JACC Cardiovasc Imaging. 2021;14(5):1068-1070. doi:10.1016/j.jcmg.2020.09.040
30. Kim HY, Lim HS, Doh JH, et al. Physiological severity of coronary artery stenosis depends on the amount of myocardial mass subtended by the coronary artery. JACC Cardiovasc Interv. 2016;9(15):1548-1560. doi:10.1016/j.jcin.2016.04.008
31. Nurmohamed NS, Danad I, Jukema RA, et al; CREDENCE and PACIFIC-1 Investigators. Development and validation of a quantitative coronary CT angiography model for diagnosis of vessel-specific coronary ischemia. JACC Cardiovasc Imaging. 2024;17(8):894-906. doi:10.1016/j.jcmg.2024.01.007
32. Strepkos D, Alexandrou M, Mutlu D, et al. TCT-382 Quantification of myocardial mass supplied by the side branch and main vessel of patients undergoing bifurcation pci using the Heartflow analysis of coronary computed tomography angiography and association with clinical outcomes. J Am Coll Cardiol. 2025;86(17_Supplement):B168. doi:10.1016/J.JACC.2025.09.493
33. Carvalho PEP, Cavalcante JL, Lesser J. Coronary CTA-guided bifurcation PCI: role of FFRCT virtual PCI and myocardial mass for preprocedural planning. JACC Case Rep. 2025;30(2):102814. doi:10.1016/j.jaccas.2024.102814
34. Precise Procedural and PCI Plan (P4) (P4). ClinicalTrials.gov identifier: NCT05253677. Updated January 1, 2026. Accessed April 17, 2024. https://clinicaltrials.gov/study/NCT05253677














