CHAMPION-AF: 3-Year Results and Implications for the Future of Left Atrial Appendage Closure
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
In this interview with the Journal of Invasive Cardiology, Matthew Sherwood, MD, discusses how the 3-year results of the CHAMPION-AF trial support left atrial appendage closure (LAAC) with WATCHMAN FLX™ (Boston Scientific) as a safe, effective, and lower-bleeding alternative to long-term oral anticoagulation for many patients with atrial fibrillation (AFib), with the potential to expand use further as guidelines, reimbursement, and longer-term data evolve.
What do the positive CHAMPION-AF trial results represent in the evolution of LAAC, and why is it an important moment for the field?
It’s really important to see that CHAMPION-AF, as designed, was able to meet both of its primary endpoints: over 3 years, in lower-risk patients than in previous trials, the WATCHMAN FLX™ Left Atrial Appendage Closure Device (Boston Scientific) looks like it’s a viable alternative to oral anticoagulation in the long term. That’s very helpful because in the future, that may lead to expansion of the indication for this device to patients who may not have as much bleeding risk as previously thought—patients who might be candidates for longer-term oral anticoagulation but would prefer not to be. Obviously, we’ll see what the guideline writers and different authorities eventually say, but I think the data supports consideration of WATCHMAN FLX as an alternative for these patients.
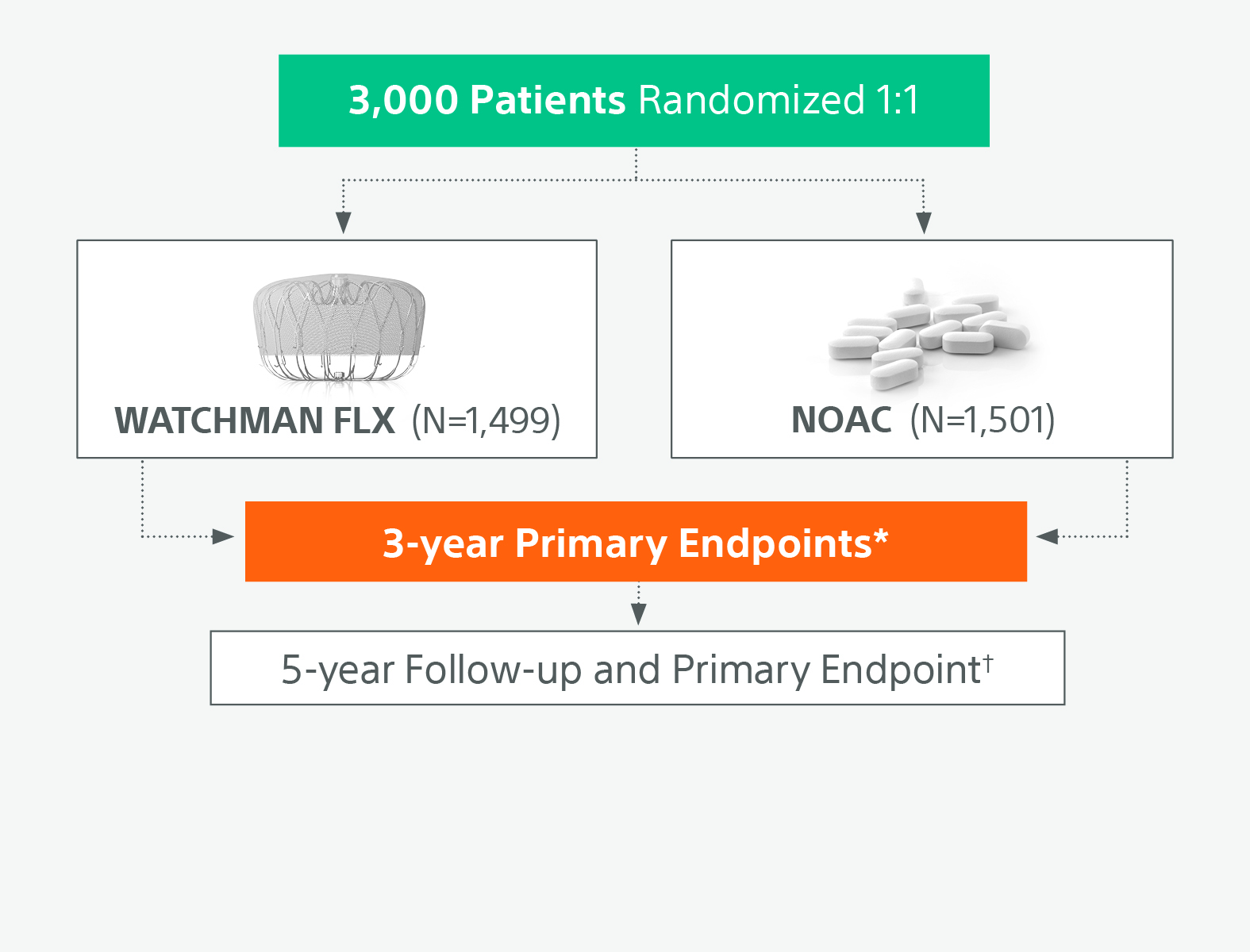
†5-year primary endpoint is non-inferiority for the occurrence of ischemic stroke or
systemic embolism
Can you comment on the primary endpoint outcomes and the net clinical benefit endpoint, and how do you consider those when weighing options for patients?
In terms of the primary efficacy endpoint looking at cardiovascular death, stroke, or systemic embolism, it’s reassuring that a procedure with the WATCHMAN FLX device is statistically as effective as using a direct-acting oral anticoagulant. Obviously, those are the most frequently used drugs across the world for patients with AFib, and seeing that it can be effective in that same way is very reassuring. What we will wait to see is if that extends to 5 years, because that’s really important.
In terms of the safety endpoint, this is something that we as operators have known for quite a while, and that is that this procedure is incredibly safe, and I do believe that it provides the benefit to patients of not having bleeding be a big part of their lives. We saw that modified bleeding (ie, any bleeding that required medical intervention or increased level of care) was significantly lower in the LAAC group. Imagine going to the emergency department or having to go to an office to change your medical therapy or get a procedure done; that’s pretty serious, and I think patients will very much appreciate that being decreased with the WATCHMAN device.
CHAMPION-AF used a modified definition of ISTH clinically relevant non-major bleeding. Can you comment on that definition, and (A) why it’s important in interpreting the results, and (B) why are these types of bleeds still relevant for patients?
They used a modified ISTH [International Society of Thrombosis and Haemostasis] definition for clinically relevant non-major bleeding: it had to be bleeding that was serious enough to require seeking medical attention, including hospitalization, but didn’t fall under the rubric of major bleeding. So, in this case, I think it’s actually pretty rigorous in terms of an endpoint because it wasn’t just “I talked to my doctor about it over the phone, or I sent a message in,” etc. You had to have had a hospitalization, medical intervention, or increased level of care per this definition. That’s a high bar that makes this more clinically important for patients. If you can reduce that for patients, I think it makes a significant clinical difference.
Given the evolving evidence base, how are you currently selecting patients for WATCHMAN implantation, and how will this shift in light of CHAMPION-AF?
Currently, I am very much a person who wants to provide benefit to patients and follow the guidelines. I am careful to evaluate and document cases that have multiple reasons for not being a good candidate for long-term oral anticoagulation. First, most of the patients that come to me are indeed at moderate-to-high risk for stroke; we usually calculate that by CHA₂DS₂-VASc score, so it’s not incredibly often that I receive a patient that doesn’t have high enough risk for stroke. What I’m usually identifying is their risk for bleeding, and the rationales for not wanting to be on long-term oral anticoagulation, including bleeding, fall risk, occupational risk, or non-adherence, for example. That’s where I currently am in treating patients.
I do think that the CHAMPION-AF results provide an opportunity to expand that indication to patients that are good candidates for oral anticoagulation but simply, for one reason or another, prefer not to take them long term. I have not started with that expansion in my practice because I certainly want to see how the guideline writers and other professional societies react to this data, as well as a potential labeling change by the FDA.
Also, I think it’s very important for all clinicians to realize that we will follow up and make sure that these procedures will be reimbursed with prior authorization, not only for our hospital’s sake but also for the patient’s sake. We don’t want it denied because we’re doing something so far ahead of the curve that it won’t be reimbursed. But for now, my practice is starting to look at those patients and say, “I really think this could be an option in the near future ”.
How do trials like CHAMPION‑AF shape conversations with patients on non-vitamin K antagonist oral anticoagulants (NOAC) around stroke protection options, particularly when balancing risks and benefits from available therapies?
What I discuss with patients is that if you can tolerate an oral anticoagulant, they have the most data in terms of protection against stroke. But if for any reason you can’t tolerate that drug, we have a great alternative in LAAC with WATCHMAN. Now, in this case, what I tell patients is “look, there may be an option that provides similar protection from stroke with less bleeding, and we have 3-year data on it that looks very favorable. If that’s something that you’re interested in, I think that’s something we could consider for you in the near future.”
I’ll also mention to them that if they’re worried about the longer term, we will have 5-year data soon to confirm long-term protection. So, I really like to give patients the option and be very open about the data that we have.

Which patient profiles stand to benefit most from earlier consideration of LAAC?
We certainly understand that patients at high risk for bleeding—which may include clinically relevant bleeds, particularly recurring ones—should be consulted as soon as possible because WATCHMAN is a great opportunity for those patients to be protected and to reduce their risk of stroke while reducing the risk of bleeding. I think we can clearly see that there is a reduction in significant bleeding for those patients, and that’s a positive outcome for patients like that. For lower-risk patients who are tolerating their oral anticoagulation but may struggle with 100% adherence to therapy, I think WATCHMAN could provide an option for a one-time procedure instead of lifelong medical therapy, but I do want to see longer-term data to understand exactly what to do with my lowest-risk patients.
CLOSURE‑AF also generated significant attention with its comparison of LAAC to medical therapy. How do you interpret those findings alongside CHAMPION‑AF, and what should clinicians take away when looking at both studies together?
CLOSURE‑AF was a single country study out of Germany. If you look at the CHA₂DS₂-VASc scores and those things, CLOSURE‑AF was a higher-risk population with respect to stroke and bleed risk when compared with the CHAMPION-AF population.
One thing that stood out to me in CLOSURE‑AF was that instead of using all WATCHMAN FLX (as in CHAMPION-AF’s case), CLOSURE‑AF used devices that have not been proven to be—I think—as safe as WATCHMAN FLX is in over 50% of patients; they used a lot of Amulet, even some WATCHMAN 2.5 and LAmbre devices. And so, in that case, what we saw was that the adverse events with the device, and bleeding specifically, were much more common in the CLOSURE‑AF population than in the CHAMPION-AF population where you saw incredible safety for the procedure. I think that has to change how we look at those results, because I think that’s where the major difference there lies.
What differences in trial design, patient population, or endpoint definitions between CHAMPION-AF and CLOSURE-AF are most important when interpreting the data?
Overall, when we’re looking at the design, etc, I think we’re really looking at the patient selection. Clearly, patients were higher risk in CLOSURE-AF, and that’s significant. There’s no doubt when we look at those higher-risk patients, we just have to be mindful of what that means.
Another thing that comes to mind is, as I’ve said, the difference in the devices used. I think that’s really important because, for example, given that the Amulet device and the WATCHMAN 2.5 device were used, rates of bleeding, including pericardial tamponade, were significantly higher in CLOSURE‑AF than they were in the CHAMPION-AF group. That can sway the major bleeding endpoint, which was where we saw an excess
in CLOSURE‑AF as compared with the CHAMPION-AF trial.
One of the other things that is different in CLOSURE‑AF is that they used dual antiplatelet therapy (DAPT) for 80% of their patients as the post-implant regimen. I think it’s important because what we’ve seen with DAPT is, when compared with oral anticoagulation alone, DAPT is probably associated with more major bleeding, and that can impact the results as we follow high-bleeding-risk patients, as we saw here.
If we look at, for example, stroke rates, those were similar between the groups, which reaffirms the mechanistic intent of LAAC. That’s reassuring because that is very much like what we saw in CHAMPION-AF; although, the stroke rates were slightly higher.
From an implanter’s perspective, do you anticipate CHAMPION‑AF influencing referral patterns, multidisciplinary collaboration, or how health systems as a whole think about stroke protection strategies over time as reimbursement and guidelines change?
That’s a difficult question. There are multiple parts to it, but I do think that as data from CHAMPION-AF, and as other data, accumulate, this will fundamentally change who is referred to providers that provide LAAC. I think we’ll start seeing lower-risk patients and possibly patients who don’t have bleeding problems, don’t have a major problem with long-term anticoagulation but for one reason or another want to be off of those drugs. We’ll start to have that conversation more with those patients concerning this data.
In terms of health systems, that will only increase the need for us to be very efficient with these procedures and to be able to provide the procedures to more patients in a clinically efficient way. This trial, along with OPTION, provides the opportunity to possibly do this procedure in a concomitant workflow with AFib ablation, which we’ve seen increase already in the United States. So, we may see more of that option used for patients who want a full solution for their AFib risk: to reduce their risk of symptoms, and also to reduce their risk of stroke. A combined procedure may be beneficial to those patients. Time will tell how frequently that will be used, but I think health systems definitely have to take that into consideration.
Based on the totality of evidence, where do you see WATCHMAN fitting into the AFib stroke risk‑reduction landscape over the next several years?
I believe WATCHMAN will be a critical component to stroke-risk reduction for AFib patients, and certainly for reducing the risk of bleeding when compared with medications. I think we’ll see this continue to emerge as a therapy that’s used more frequently, and I believe that this will lead to using this in patients who are at lower risk in the near future.
What would you say to your peers who may still be skeptical of LAAC therapy, even within today’s patient indication that is unable to tolerate long-term anticoagulation, based on the results of CHAMPION-AF?
I would say that I understand that people want to feel safe and want to see that things are as effective as the medications we’ve been using for a long period of time. But I would encourage them to look into it because I do believe that there’s very good data to indicate that LAAC with the WATCHMAN FLX device provides benefit to patients, especially those who have bleeding problems or who either can’t take, have frequent interruptions to, or are non-adherent with their oral anticoagulants. That’s very important to offer to patients, because I think if you have a sit-down discussion with patients who have bleeding problems, or falls, or other issues, this is an important option that they need to be presented with.
In the future, it may be that this is a reasonable option for patients even if they don’t have bleeding problems, and so it should be a discussion that is offered to those patients if the indication changes. That means that many patients may choose not to have this procedure, but they should at least have it as an option.
The transcript has been lightly edited for clarity.
Disclosures: Dr Sherwood reports modest (<$5000) consulting honoraria from Boston Scientific and Abbott, and significant (>$5000) consulting honoraria from Medtronic.
This content was published with support from Boston Scientific. Permission for use of the figures was granted by Boston Scientific. SH-2516911-AA