Unmasking the True Culprit in ST-Segment Elevation Myocardial Infarction With Coronary Artery Aneurysm
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00086. Epub April 13, 2026.
Coronary artery aneurysms can complicate the management of ST-segment elevation myocardial infarction (STEMI), as altered flow patterns and a large thrombus burden may obscure the true culprit lesion on angiography.1,2
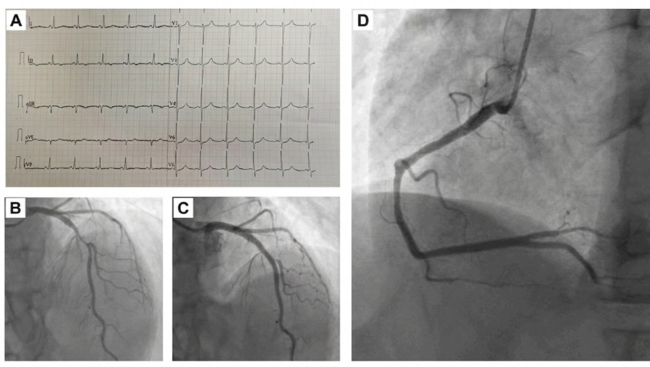
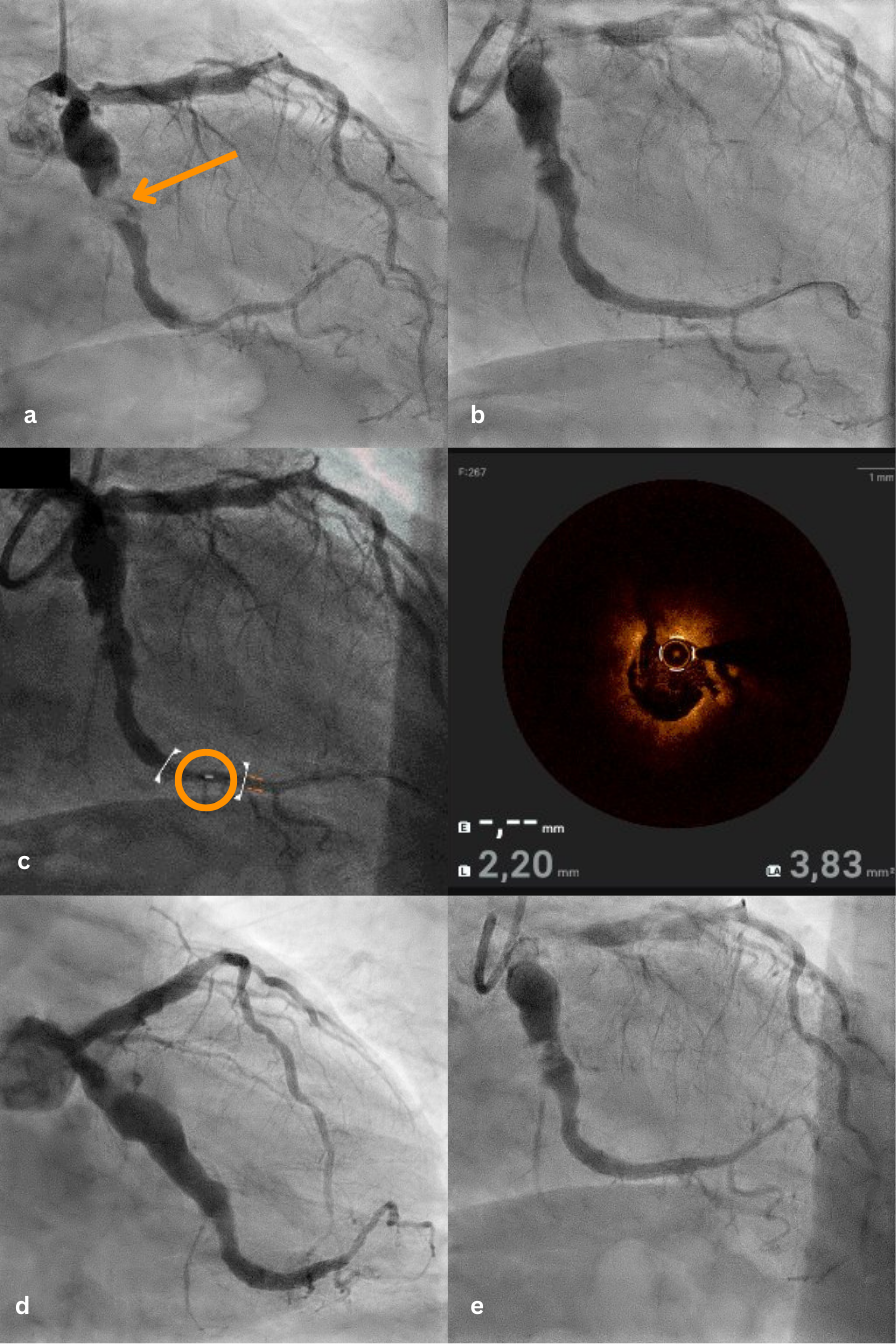
A 76-year-old male with a history of arterial hypertension and hypercholesterolemia, but no known coronary artery disease, presented with typical chest pain. Electrocardiography showed ST-segment elevations in leads II, III, aVF, and V6. Emergent coronary angiography revealed a markedly aneurysmatic (>6 mm) circumflex artery with massive proximal thrombotic occlusion and preserved distal vessel caliber (Figure A).
Based on angiographic appearance, the aneurysmal segment was initially suspected as the culprit lesion. Thrombus aspiration followed by balloon dilatation partially restored flow (Figure B). Given the ambiguous angiographic findings and complex anatomy, optical coherence tomography (OCT) was performed. OCT demonstrated a large amount of red thrombus within the proximal aneurysmal segment and revealed the actual culprit lesion: a distinct plaque rupture in the distal, non-aneurysmatic circumflex artery (Figure C, Video). These findings suggested secondary thrombus propagation from the distal rupture site into the aneurysm rather than primary rupture within the aneurysmal segment.
Based on this imaging-guided diagnosis, percutaneous coronary intervention was performed with implantation of 2 drug-eluting stents limited to the distal culprit lesion, deliberately avoiding stent placement within the aneurysmal segment. Final angiography showed optimal stent expansion and Thrombolysis in Myocardial Infarction 3 flow (Figure D). The patient received intensive antithrombotic therapy including intracoronary and intravenous tirofiban in addition to dual antiplatelet therapy. Follow-up angiography after 8 weeks demonstrated sustained vessel patency and stable aneurysm morphology (Figure E).
This case highlights the incremental value of intracoronary imaging in complex STEMI scenarios. In the presence of coronary artery aneurysms, angiography alone may be misleading. OCT can identify the underlying plaque pathology and guide a more targeted revascularization strategy, potentially avoiding unnecessary stent implantation in aneurysmal segments.
Affiliations and Disclosures
Elaaha Anwari, MD1,2; Fardin Hamidi, MD1; Denitsa Meteva, MD1,2; Ulf Landmesser, MD1,2,3; Youssef Abdelwahed, MD1,2,3
From the 1Department of Cardiology, Angiology and Intensive Care Medicine, Deutsches Herzzentrum der Charité, Campus Benjamin Franklin, Charité University Medicine Berlin, Berlin, Germany; 2Friede Springer Cardiovascular Prevention Center @Charité, Berlin, Germany; 3German Center for Cardiovascular Research (DZHK), Partner Site Berlin, Berlin, Germany.
Disclosures: Prof Dr Landmesser reports research support to his institution from Abbott, Amgen, Bayer, and Novartis outside of this work. Dr Abdelwahed has received consulting fees from Boston Scientific and Shockwave outside of this work. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that witnessed verbal consent for submission and publication of this case report, including images and associated text, has been obtained from the patient.
Address for correspondence: Elaaha Anwari, MD, Department of Cardiology, Angiology and Intensive Care Medicine, Deutsches Herzzentrum der Charité, Campus Benjamin Franklin, Charité University Medicine Berlin, Hindenburgdamm 30, Berlin 12203, Germany. Email: elaaha.anwari@dhzc-charite.de; X: @elaaha_a
References
1. Swaye PS, Fisher LD, Litwin P, et al. Aneurysmal coronary artery disease. Circulation. 1983;67(1):134-138. doi:10.1161/01.cir.67.1.134
2. Byrne RA, Rossello X, Coughlan JJ, et al; ESC Scientific Document Group. 2023 ESC guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44(38):3720-3826. doi:10.1093/eurheartj/ehad191