Thrombus Migration From the Left Circumflex to the Distal Left Anterior Descending Artery During Primary Percutaneous Coronary Intervention: An Unexpected Complication
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00095. Epub April 9, 2026.
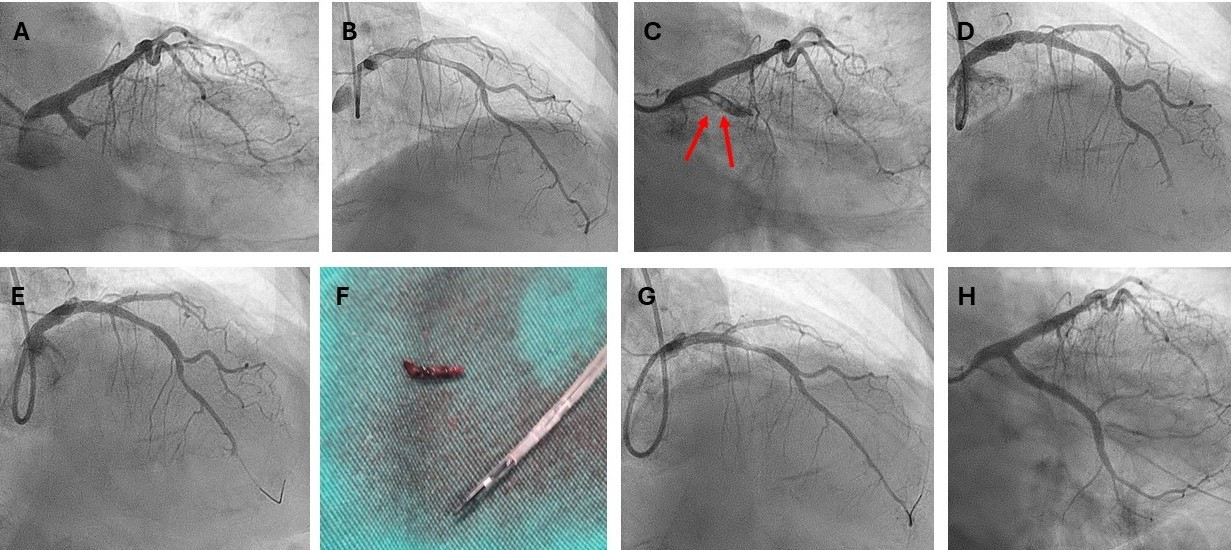
An 82-year-old woman with a high-risk non-ST-elevation myocardial infarction (NSTEMI) was admitted. Urgent coronary angiography revealed a proximal left circumflex (LCx) total occlusion with a very high thrombus burden (Figure A, Video 1), a super-dominant right coronary artery (RCA), and an unobstructed left anterior descending artery (LAD) (Figure B).
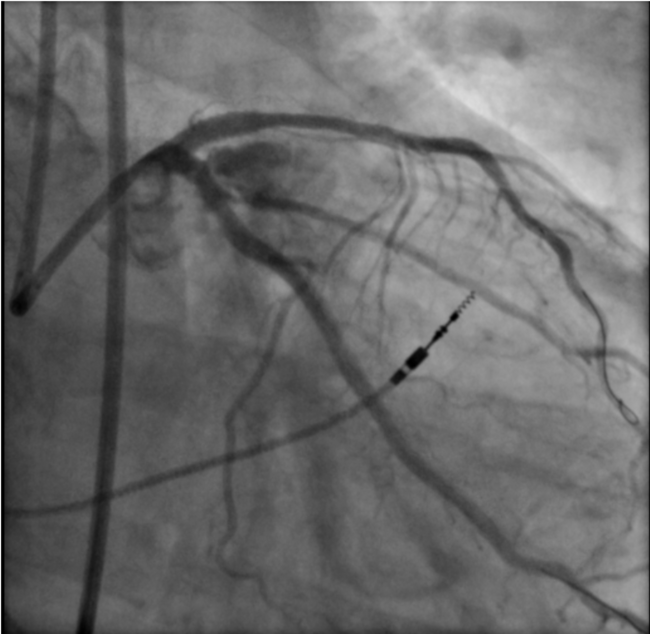
Multiple attempts to cross the occlusion using a SAMURAI workhorse guidewire (Boston Scientific) were unsuccessful; therefore, a Sion Blue guidewire (ASAHI INTECC) was selected for further attempts. While both guidewires were positioned in proximal LCx, 2 thrombi were visualized in the proximal LCx segment (Figure C, Video 2).
Despite gentle contrast injections, the thrombi migrated into the LAD, resulting in distal LAD occlusion (Figure D, Videos 3 and 4). The LAD was then wired with the Sion Blue guidewire, which was advanced into its distal segment (Figure E). An intracoronary bolus of tirofiban failed to improve the angiographic appearance of the LAD; therefore, thrombus aspiration was performed using a Thrombuster II device (Kaneka Medical). A large thrombus was successfully aspirated (Figure F), immediately restoring LAD flow (Figure G). A new Sion Blue was used to finally cross the LCx occlusion and, following multiple predilatations, a long drug-eluting stent was deployed, achieving a nice final angiographic result (Figure H). The patient had an uneventful recovery.
Thrombus migration during percutaneous coronary intervention is uncommon but can lead to serious complications. In such cases, thrombus aspiration is essential for restoring coronary flow. In cases of proximal LAD or LCx occlusion with a high thrombus burden, prophylactic wiring of the other coronary artery may be a reasonable strategy. This approach could prevent difficulty in crossing the vessel if a large thrombus migrates and becomes lodged at its ostium, a situation that may make wiring impossible and could potentially lead to catastrophic consequences for the patient.
Affiliations and Disclosures
Konstantinos C. Theodoropoulos, MD, PhD; Matthaios Didagelos, MD, PhD; Charalampos Kakderis, MD; George Kassimis, MD, PhD; Antonios Ziakas, MD, PhD
From the 1st Cardiology Department, AHEPA University Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the interventions described in the manuscript and to the publication of their data.
Address for correspondence: Konstantinos C. Theodoropoulos, MD, PhD, 1st Cardiology Department, AHEPA University Hospital, Aristotle University of Thessaloniki, Thessaloniki 546 36, Greece. Email: ktheod2005@hotmail.com; Instagram: @ktheod2005; X: @ktheod2005