


Anatomical Variants in Foot and Ankle Surgery: Avoiding Missed Diagnoses, Surgical Pitfalls, and Recurrence
Anatomical variants can dramatically alter surgical planning and outcomes in foot and ankle procedures, yet many remain underrecognized. From metatarsus adductus complicating hallux valgus reconstruction to unpredictable nerve pathways and accessory ossicles, subtle differences in anatomy often demand major intraoperative pivots. In this expert interview about his ACFAS ASC session, Dr. Catanzariti explores the variants surgeons most commonly overlook and the clinical mindset required to avoid recurrence, instability, and iatrogenic injury.
Key Takeaways
1. Metatarsus Adductus Can Undermine Hallux Valgus Correction. Profound metatarsus adductus (MA) may physically prevent adequate lateral translation of the first metatarsal during bunion reconstruction. Failing to address MA, often via second and third tarsometatarsal arthrodesis or base osteotomies, can lead to compromised correction and high recurrence rates.
2. Intraoperative Discovery of Bony Variants Requires Immediate Strategy Shifts. Variants such as an os subfibulare encountered during Broström procedures can compromise anchor fixation and bone stock. Surgeons must be prepared to adjust fixation techniques, relocate anchors, or transition to non-anatomic repair methods when bone quality is insufficient.
3. “Textbook Bias” Leads to Soft Tissue and Neurovascular Complications. Early-career surgeons often underestimate variability in structures like the superficial peroneal nerve or accessory muscle bellies. Recognizing that standard anatomy represents an average - not a rule - is essential to avoiding iatrogenic nerve injury, missed pain generators, and unnecessary surgery.
In your surgical experience, which anatomical variants have you found to be most clinically significant—and most likely to be overlooked—in foot and ankle surgery?
One of the most clinically significant—and frequently underestimated—anatomic variants is metatarsus adductus (MA) in the setting of a symptomatic hallux valgus deformity.
A profound MA deformity has massive clinical implications during hallux valgus reconstruction. It is virtually impossible to adequately address a medial bunion deformity with an osteotomy or arthrodesis designed to reduce the intermetatarsal angle when the lesser metatarsals are physically blocking the way. If the surgeon is not careful, they will run out of room to laterally transpose the first metatarsal.
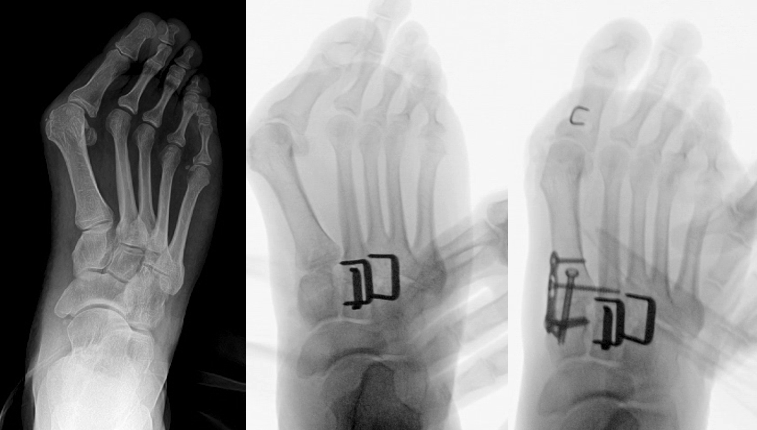
Surgical management in this situation requires a mindset shift: we must address the metatarsus adductus before proceeding with the hallux valgus reconstruction. By performing osteotomies of the second and third metatarsal bases, or my preference, arthrodesis of the second and third tarsometatarsal articulations (see photos), we effectively move the lesser metatarsals laterally. This creates the necessary real estate to correct the first ray. While this approach significantly increases operating room time and extends the patient's postoperative convalescence, failing to recognize and treat the MA essentially guarantees a compromised outcome and high recurrence rate.
How do anatomical variants most commonly alter your intraoperative decision-making, even when preoperative planning appears straightforward?
Fortunately, with a combination of clinical examination, standard radiography, and targeted advanced imaging, we can identify the vast majority of anatomic variance prior to surgery. Nonetheless, there are times when these variants reveal themselves on the table and force an immediate pivot in strategy.
A prime example occurs during lateral ankle stabilization (eg, a Broström procedure) for chronic ankle instability. Even with a preoperative MRI, we sometimes encounter unpredicted bony variants or chronic avulsion fragments incorporated into the distal fibula, such as an os subfibulare.
These bone fragments are pain generators that need to be excised, but more importantly, they are not stable enough to support the soft tissue anchors typically used for stabilization. Removing them often leaves a void or compromised bone stock. When this happens, I have to alter my fixation strategy on the fly. This might mean placing anchors in a more proximal location, utilizing larger diameter anchors, or abandoning anchors altogether in favor of a nonanatomic repair utilizing a drill tunnel to accommodate the tendon.
In your opinion, where do surgeons, particularly those earlier in their careers, tend to underestimate the impact of anatomical variability?
I find that early-career surgeons most often underestimate variability in soft tissue structures and neurovascular pathways, largely due to what I call 'textbook bias.'
We are taught standard 'safe zones' for incisions and standard locations for tendons. However, anatomical reality is often different. For example, the branching of the superficial peroneal nerve (SPN) is highly variable, and assuming it always follows the textbook illustration can easily lead to iatrogenic entrapment or neuroma during routine surgery.
Additionally, anomalous muscle bellies, such as a peroneus quartus or an accessory soleus, can crowd anatomical compartments. An inexperienced surgeon might mistake an accessory muscle for a soft tissue mass on an MRI or fail to recognize it intraoperatively as a source of tendon stenosis and retro-malleolar pain. Recognizing that 'standard anatomy' is simply an average, not an absolute rule, is a key milestone in surgical maturity.
What do you hope surgeons will approach differently in their day-to-day practice after attending your ACFAS lecture on anatomical variants?
Ultimately, my presentation is a high-level review of anatomy, but the core takeaway is about clinical correlation. We generally know where accessory bones, sesamoids, and anomalous muscles are located. The true clinical art lies in two steps: identifying the variant and critically determining whether it is an innocent bystander or the primary pain generator responsible for the patient’s symptoms.
I hope surgeons leave the lecture with a renewed commitment to treating the patient, not the radiograph. It is easy to fall into the trap of seeing an accessory navicular or an os trigonum on an X-ray and immediately attributing all the patient's medial or posterior ankle pain to it. I want them to approach their day-to-day practice by slowing down, utilizing targeted physical exams, and employing diagnostic injections to definitively prove that a variant is symptomatic before taking the patient to the operating room.
Dr. Catanzariti is the Director of the Foot and Ankle Residency Program at West Penn Hospital, Allegheny Health System, in Pittsburgh, PA.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.






