


Complications of Minimally Invasive Bunion Surgery Using a Single-Screw Fixation Technique
As minimally invasive (MIS) bunion surgery continues to gain traction, variations in fixation strategy have prompted renewed discussion around complication profiles. This article reviews both established and evolving complications associated with one-screw MIS bunion correction and offers insights for prevention and management.
Key Takeaways
- Technique and experience matter more than screw count. Many complications associated with single-screw MIS bunion surgery are strongly linked to surgical execution and the steep learning curve, with complication rates declining as surgeon experience increases.
- Unique and emerging complications deserve attention. Metatarsal explosion patterns, metatarsal head disengagement, and latent dorsal head displacement appear to be technique-related phenomena that may occur even with proper execution and may warrant consideration of 2-screw constructs in some patients.
- Patient risk stratification is essential. While 1-screw fixation can be successful, patients with higher risk factors for nonunion or instability—and surgeons early in their MIS experience—may benefit from a 2-screw approach until the establishment of clearer guidelines and longer-term evidence is available.
Minimally invasive surgery (MIS) for bunion deformities has become increasingly popular over the past few years. In recent times, the original MIS first metatarsal osteotomy technique with screw fixation was described with a 2-screw construct. Currently, some surgeons are fixing the first metatarsal osteotomy using a 1-screw technique. Each technique is not without potential complications. With the 1-screw technique, these complications can vary widely. This article explores potential complications associated with minimally invasive bunion correction while utilizing a single screw technique.
All surgeries are not without risk of complications. Minimally invasive bunion surgery is thought to reduce risk of certain adverse events such as incision dehiscence or infection; however, this approach is still susceptible to complications following the procedure.1
According to literature, the most common complications associated with MIS bunion correction are joint stiffness and recurrence. Lonati, in a systematic review, suggested stiffness and recurrence were the most common complications.2 Miranda noted joint stiffness following MIS bunion correction at 18.47% and recurrent hallux abductovalgus HAV at a rate of 15.2%.3
De Prado also cited a complication rate of burns to the skin at 0-13% of cases. De Prado noted that as surgeon experience grew in their surgical technique, this rate of skin burns decreased.1
Other complications seen in both MIS and open bunion surgery include infection, burr-related nerve injury, hallux varus, malunion, complex regional pain syndrome (CRPS), hardware irritation, fracture, and avascular necrosis (AVN).1
Many of the complications in literature are quoted as due to improper execution of surgical techniques, as MIS bunion correction does have a steep learning curve.4 These complications decrease in rate as surgeon experience increases. Merc noted that it takes approximately 30 cases for a surgeon to become comfortable with the procedure, leading to a decrease in operating room (OR) time, fluoroscopy time, and postoperative complications.5 This pattern of complication improvement may also overlap with patterns seen as surgeons advance their comfort with open procedures.
Other complications of MIS bunion procedures are transfer metatarsalgia, nonunion, malunion, first metatarsal shortening, and hardware removal or failure.6 Another particularly interesting complication specific to MIS bunion surgery is metatarsal explosion. Baskin and colleagues developed a fracture classification and treatment system with 3 fracture patterns that may occur as a complication to MIS bunion correction.7
What is Metatarsal Explosion?
The first classification, Type 1 metatarsal explosion, is identified by a pathognomonic “fleck fracture” seen on a dorsoplantar radiograph. The fleck fracture is a distal lateral fracture of the first metatarsal. This fracture occurs between the metatarsals at the lateral aspect and is thought to be associated with an exit point of the intramedullary screw that is too close to the osteotomy, thus causing a stress fracture. This is the most common fracture pattern for this complication at 50%.7
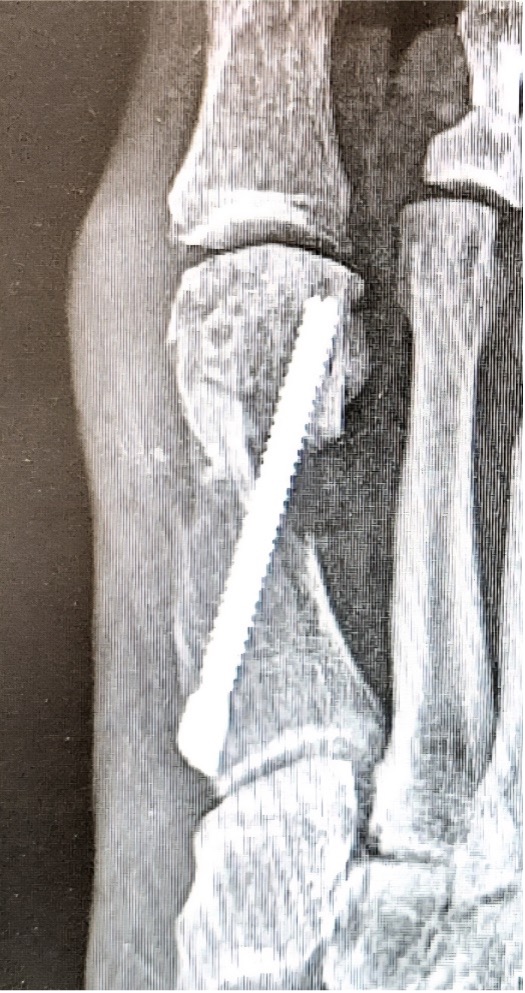
The second type of metatarsal explosion is identified by a pathognomonic “double metatarsal sign.” This explosion pattern is a complete through-and-through fracture of the first metatarsal. The fracture is split into 2 pieces along the transverse plane, extending into the tarsometatarsal joint, creating an illusion of 2 metatarsals on an AP radiograph. The prevalence of this type of metatarsal explosion is 31%.7 Figure 1 displays a Type 2 metatarsal explosion.
The third type of metatarsal explosion is the most catastrophic, identified by a large detached “butterfly fragment.” The Type 3 explosion has multiple fracture fragments that travel along the plane of fixation, similar to Type 2 explosions, but is extra-articular and does not exit the first metatarsal-cuneiform joint. The fragments form a dorsal butterfly fragment that is the hallmark appearance of this fracture type. Type 3 is the rarest at 19% and the most often requiring revision surgery.7
One of the main factors associated with metatarsal explosions was felt to be technique driven; either placing the screw too close to the osteotomy, in the case of Type 1 explosions, or inserting the screw at an angle excessively dorsiflexed or plantarflexed, as seen in the other explosion types. However, the complication also occurred in the setting of flawless technique. Despite being an uncommon complication, it is thought to be an inevitable one. There was no significant difference in preventing metatarsal explosions between 1- and 2-screw techniques.7

Notes on Nonunion
Nonunion is also a complication that can be difficult to manage. Genuth and colleagues reported a nonunion rate of 0.3%, or 17 cases in their series.8 They found this to be consistent with previous study findings and did not identify any unique clear risk factors in their series.8
However, general risk factors for nonunion after MIS bunion surgery are multifactorial and include surgical technique; patient comorbidities such as endocrine abnormalities, low vitamin D status, smoking, poor nutrition and patient medications, such as oral steroids.9,10
In an attempt to prevent reoperation for nonunions, one may attempt traditional treatments such as smoking cessation, bone stimulators, and/or dietary supplementation. Timing as to when to perform a revision surgery is controversial and has not been definitively established. However, it is the authors’ opinion that traditional symptoms such as unrelenting pain and difficulty walking after 3-6 months after surgery without radiographic signs of union are reasonable indications. If the patient’s nonunion is asymptomatic, and the hardware is in good position, it is possible to wait up to 12 months prior to attempting revision surgery.
In Figures 2 A, B, C one can see an example of a nonunion at 1 year that required revision surgery. The patient used a bone stimulator for 6 months, and ultimately went on to revision surgery at 13 months postoperative from the index MIS bunion surgery. This was an example of a successful revision surgery, removing the initial hardware, utilizing an autogenous tricortical bone graft from the calcaneus, and a dual plating construct.

Pointers on Postoperative Protrusions
Another complication that can occur is the presence of a symptomatic bump on the medial side of the foot, proximal to the osteotomy at the metatarsal neck. Other causes of potentially symptomatic protrusions include reoccurrence or proud hardware that gives the impression of a painful bump. Although rare, this can be a source of pain when wearing shoe gear. These complications may result from inadequate resection of the residual medial spike of bone of the metatarsal shaft created when translating the metatarsal head laterally. In addition, when screw placement is improperly placed too distal or too proud in the metatarsal shaft, this complication may result. As the surgeon gains experience and confidence, this is much less of an issue. However, it still can occur with proper technique regardless of using a 1- or 2-screw technique.
In Figures 3 A, B, C, D, the images depict the case of an elderly female who previously underwent a MIS bunion surgery. Unfortunately, she experienced a recurrent HAV and painful proximal hardware medially (Figures 3 A, B). She subsequently underwent hardware removal and revisional MIS bunion surgery (Figure 3 C, D).

Other Unique Complications to Consider
Disengagement of the metatarsal head is another complication discussed in a lecture at the Annual Scientific Conference of the American College of Foot and Ankle Surgeons in Phoenix in 2025.11 It can occur during the first few weeks postop. It is characterized by complete uncoupling of the first metatarsal head (pulling of the screw through the cortex) with complete loss of correction, without failure or movement of the hardware. This complication may or may not be symptomatic, but almost always requires revision (Figures 4 A, B).

Ectopic bone formation associated with MIS bunion surgery is a rare complication that surgeons discuss, but as of yet is not reported in the literature. The condition may be confused with a proximal bump, but is distinctly unique. This can occur many months after surgery, sometimes even after the patient has been discharged from care. The patient presents with identical symptoms of a proximal bump despite normal radiographs. It does not appear to be technique-related, but may be due to the robust bone callus formation that occurs during bone healing. Surgical treatment is often delayed for several months in the hopes that the bone will remodel with time (Figure 5).

Another discussed complication not yet reported in the literature is latent dorsiflexion displacement of the head of the first metatarsal (LDDH). This can occur once weight-bearing starts, but is often seen after 6 weeks when the patient is back into regular shoe gear. While it may be asymptomatic, the symptomatic patient will complain of a dorsal bump, lesser metatarsalgia, and joint stiffness (Figures 6 A, B, C, D). Author EB has only seen this occur when using a single-screw technique. The authors believe this complication can be reduced with the use of a 2-screw construct to prevent instability. Further research into LDDH is necessary to avert these types of malunions.

Burr-induced nerve-related injury is also a potential complication that concerns some surgeons as they wade through their learning curve. In our experience, this complication and others may have been overstated, as burr technology, techniques, and MIS education has improved. A likely reason for this is that the original technique called for the use of a 3.1 mm wedge burr to remove/pulverize the “medial spike.” While this can be an efficient technique, we find that the wedge burr is more inclined to grab soft tissue and nerves than its “Shannon-type” burr counterpart. Shannon burr utilization solely to remove the medial spike via osteotomy, rasping or debridement appears to be a safer way to remove the prominence regardless of the technique. The authors have not experienced a nerve injury while using a Shannon burr. We also believe the complication contention due to burr inexperience has been exaggerated. In addition to inexperience in removing the medial spike, sometimes there is a small proximal bump. Also, improper distal screw insertion or leaving the head of the screw prominent can be causative factors. These too should also decrease with experience.


Discussion and Conclusion
Minimally invasive bunion correction surgery has become popular in recent years due to the idea that minimally invasive technique has less risk of complications, provides an easier postoperative course, better cosmesis, and facilitates a safer surgical treatment. Recently, some surgeons have begun performing the surgery using a 1- as opposed to 2-screw technique. One should expect complications in MIS bunion correction to decrease with surgeon experience, and complications can occur regardless of screw count. While a one screw technique has been proven to be safe and successful, it is not immune to its share of misfortune.
We feel that 1-screw MIS bunion surgery is safe and effective, but not without its share of complications. Steps may be taken to mitigate misadventures with a single-screw technique, but further research and education is needed. While the prospect of using a 1-screw technique is promising we believe that 2 screws when feasible may better serve patients with higher risk factors and surgeons newer to MIS, until further research and parameters have been established.
Dr. Baskin practices with Advocare Stafford Orthopaedics in Manahawkin, NJ.
Dr. DiDomenico is the Fellowship Director at Northern Ohio Medical Specialist (NOMS) Ankle and Foot Care Centers and an Adjunct Professor at Kent State University College of Podiatric Medicine.
Dr. Anain is a Fellow at NOMS Ankle and Foot Care Centers.
References
1. De Prado M. Complications in minimally invasive foot surgery. Fuss Sprunggelenk. 2013;11(2):83-94. doi:10.1016/j.fuspru.2013.02.007
2. Lonati D, et al. A multidimensional systematic review of minimally invasive bunion surgery (MIBS). J Clin Med. 2025;14(8):2757. doi:10.3390/jcm14082757
3. Miranda MA, et al. Complications on percutaneous hallux valgus surgery: a systematic review. J Foot Ankle Surg. 2021;60(3):548-554. doi:10.1053/j.jfas.2020.06.015
4. Andreas T, Strässle M. The percutaneous learning curve of third-generation minimally invasive Chevron and Akin osteotomy (MICA). Foot Ankle Surg. 2022;28(8):1389-1398. doi:10.1016/j.fas.2022.07.006
5. Merc M, et al. Learning curve in relation to radiation exposure, procedure duration, and complication rate for minimally invasive Chevron Akin (MICA) osteotomy. BMC Musculoskelet Disord. 2023;24(1):1-10. doi:10.1186/s12891-023-06706-1
6. Di Nucci KA. The unfamiliar complications of minimally invasive foot surgery. Clin Podiatr Med Surg. 2025;42(1):117-138. doi:10.1016/j.cpm.2024.09.003
7. Blitz NM, Wing DT, Baskin ES. Patterns of metatarsal explosion after new modern minimally invasive bunion surgery: a retrospective review and case series of 16 feet. J Minim Invasive Bunion Surg. 2024;1:1-8. doi:10.62485/001c.92774
8. Genuth G, Thompson R, Zeng A, Cullen N, Goldberg A, Johnson H. The management of nonunion following minimally invasive bunion surgery. Foot Ankle Surg Tech Rep Cases. 2025;5(1):100455.
9. Reddy SC, Schipper ON, Li J. The effect of chilled vs room-temperature irrigation on thermal energy dissipation during minimally invasive calcaneal osteotomy of cadaver specimens. Foot Ankle Orthop. 2022;7(4):24730114221136548. doi:10.1177/24730114221136548
10. Thomas JD, Kehoe JL. Bone non-union. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2024.
11. Baskin ES. MIS bunion complications. Presented at: Annual Scientific Meeting of the American College of Foot and Ankle Surgeons; March 27–30, 2025; Phoenix, AZ.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.






