Image

Review the novel approach of BESREMi (ropeginterferon alfa-2b) to treating polycythemia vera and delve into efficacy and safety data from key clinical trials that supported its approval as a treatment option.
Ellen K. Ritchie, MD, is an assistant professor of medicine and a member of the Leukemia Program at the Weill Cornell Medical College of Cornell University and the New York Presbyterian Hospital in New York City. Dr Ritchie graduated from Barnard College at Columbia University and received her medical degree from the College of Physicians and Surgeons at Columbia University in New York City, where she was also elected to the Alpha Omega Alpha Honor Society. She completed her internship and residency in internal medicine and her fellowship in hematology and medical oncology at New York Presbyterian Hospital, Columbia campus. Dr Ritchie's research interests are in the treatment of older patients with anemia, cytopenias, myelodysplastic syndromes, myeloproliferative disorders, and acute leukemia. She is interested in finding better therapies and supportive care strategies for older patients, particularly those with hematologic malignancies. Dr Ritchie is the principal investigator on clinical trials investigating new diagnostic techniques, supportive care strategies, and therapeutics aimed at the older patient. She collaborates with investigators in the Division of Geriatrics and Gerontology. Additionally, she has been the author or co-author of many publications.
My name is Ellen Ritchie, and I'm associate professor of clinical medicine at Weill Cornell Medical College in New York City. I am the assistant director of the leukemia program. I treat mainly myeloproliferative neoplasms, polycythemia vera, essential thrombocythemia, and primary myelofibrosis.
Welcome to the second video of our series on treatment options for polycythemia vera, or PV. In this video, we will explore the novel approach of BESREMi (ropeginterferon alfa-2b) to treating PV and delve into the efficacy and safety data from key clinical trials that supported its approval as a treatment option.
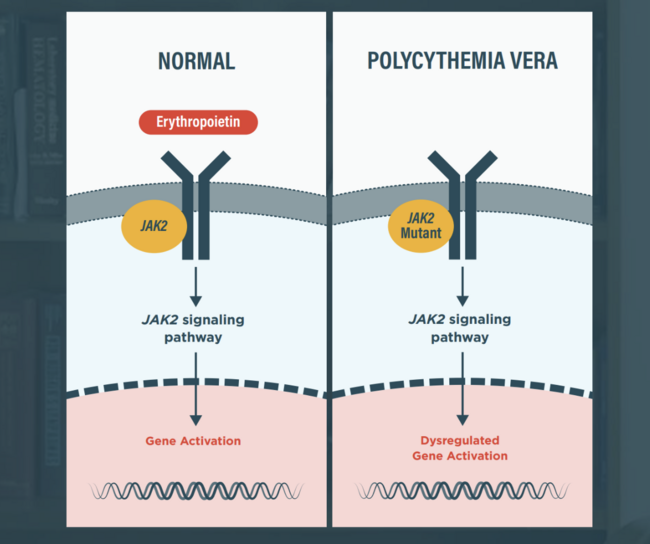
Interferon alpha (IFN
In 2021, ropeginterferon alfa-2b-njft (BESREMi), a long-acting, mono-pegylated IFN
Indications2
BESREMi is indicated for the treatment of adults with polycythemia vera.
Boxed Warning2
WARNING: RISK OF SERIOUS DISORDERS
Interferon alfa products may cause or aggravate fatal or life-threatening neuropsychiatric, autoimmune, ischemic, and infectious disorders. Patients should be monitored closely with periodic clinical and laboratory evaluations. Therapy should be withdrawn in patients with persistently severe or worsening signs or symptoms of these conditions. In many, but not all cases, these disorders resolve after stopping therapy.
Dosage and Administration2
Recommended starting dose is 100
Increase the dose by 50
Now, let’s delve into the efficacy and safety data from BESREMi’s key clinical trials.
The PEGINVERA study, a pivotal trial for BESREMi’s FDA approval, was a prospective, multicenter, single-arm trial evaluating the dosing, tolerability, and efficacy of BESREMi in adult patients with PV.4
This study, which had a duration of 7.5 years, included 51 patients with confirmed PV and JAK2 mutation, regardless of prior cytoreductive therapy. BESREMi was administered subcutaneously biweekly, starting with a 50 𝜇g dose, and titrated every 2 weeks.2
The efficacy was evaluated by assessing complete hematologic response (CHR), which was defined as hematocrit <45%, no phlebotomy in the preceding 2 months, platelets ≤400 x 109/L, and leukocytes ≤10 x 109/L.2
Eighty percent of the treated patients experienced complete hematologic response, with a median duration of 20.8 months, and 61% achieved comprehensive disease control, with a median duration of 14.3 months.2,5
Next, let’s review the safety and tolerability data from the PEGINVERA study.
Ninety-five percent of the adverse reactions reported were grade 1 or grade 2, and nearly 40% of the adverse reactions occurred in the first 3 months of the treatment.6
Sixteen percent of the patients experienced serious adverse reactions, the most common of which were urinary tract infection, transient ischemic attack, and depression.2
Adverse reactions requiring permanent discontinuation in greater than 2% of patients who received BESREMi included depression, arthralgia, fatigue, and general physical health deterioration.2
The most common adverse reactions reported in greater than 10% of patients in the PEGINVERA study over 7.5 years included influenza-like illness, arthralgia, fatigue, pruritus, nasopharyngitis, and musculoskeletal pain.2
There were no cases of AML and 1 case of myelofibrosis out of 51 patients treated with BESREMi over the 7.5 years.5,6
Additionally, evaluation of the pooled safety population of 178 patients with PV who were treated with BESREMi monotherapy in the PEGINVERA, PROUD-PV, and CONTINUATION-PV studies showed that the most common adverse reactions occurring at a rate higher than 10% were liver enzyme elevations, leukopenia, thrombocytopenia, arthralgia, fatigue, myalgia, and influenza-like illness.6
Together, these safety data supported BESREMi as a valuable treatment option for PV by demonstrating a well-tolerated safety profile with manageable side effects.
While the PEGINVERA study included both high- and low-risk PV patients, the LOW-PV study evaluated the efficacy and safety of BESREMi in low-risk adult patients with PV, defined as less than 60 years of age and no history of thrombosis.7
The LOW-PV study was a phase-2, multicenter, open-label, 2-arm, parallel-group, investigator-initiated, randomized trial comparing the efficacy and safety of BESREMi in combination with standard phlebotomy and low-dose aspirin versus phlebotomy and low-dose aspirin alone in low-risk PV patients.7
It included 127 adult patients who were randomized to either the standard group, who received phlebotomy and low-dose aspirin, or the experimental group, who received BESREMi along with the phlebotomy and low-dose aspirin. The standard group consisted of 63 patients, and the experimental group consisted of 64 patients. Patients in the experimental group received BESREMi subcutaneously every 2 weeks at a fixed dose of 100
The primary endpoint was the maintenance of the median hematocrit
The study had a duration of 12 months, at which point, patients could continue to an extension phase of up to 24 months. A crossover was allowed if the primary endpoint was not met at the end of the core 12-month period.7
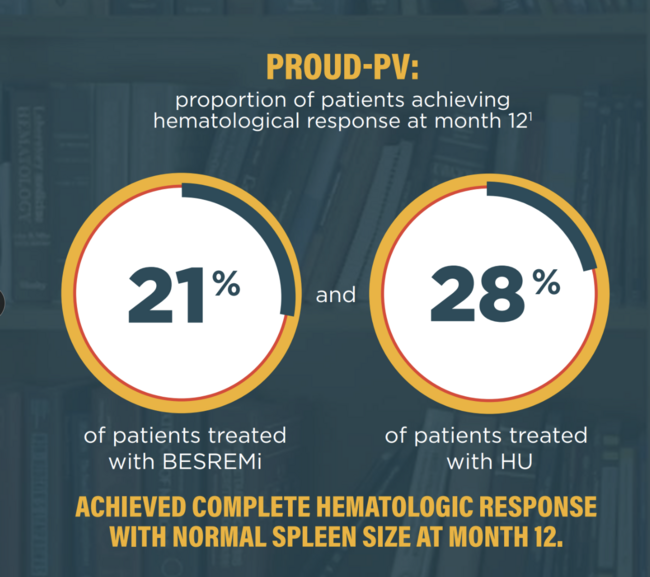
At 12 months, the composite treatment response, consisting of hematocrit control and the absence of disease progression, was achieved by 81% of the patients treated with BESREMi plus phlebotomy and aspirin, which was a significant improvement over the 51% of the patients treated with phlebotomy and aspirin alone.7
The results were similar when only hematocrit control was assessed. Eighty-one percent of the BESREMi-treated patients maintained hematocrit control compared with 59% in the phlebotomy and aspirin-only group.7
In assessing disease progression, none of the patients who received BESREMi experienced disease progression, whereas 13% of the patients in the phlebotomy and aspirin-only group showed disease progression.7
Lastly, there was a 21% reduction in the number of phlebotomies needed during the 24-month period in patients who received BESREMi plus phlebotomy and aspirin.7
In terms of safety and tolerability, grade 3 and grade 4 adverse events were reported in 9% of patients treated with BESREMi plus phlebotomy and aspirin.7
Eight percent of patients receiving BESREMi plus phlebotomy and aspirin discontinued treatment due to hypertransaminasemia, neutropenia, persistent itching, nausea/asthenia, metrorrhagia, and hyperthyroidism.6,7
In conclusion, BESREMi is a long-acting, mono-pegylated interferon, which is the only single-site mono-pegylated interferon that exhibits its cellular effects in the bone marrow.2 As efficacy and safety data from the key clinical trials demonstrate, it is capable of inducing sustained hematologic response and has a manageable side effect profile.9 Due to its longer half-life, dosing can occur every 2 weeks and is available as a subcutaneous injection.2
Thank you for joining me today as we explored the clinical trial data supporting BESREMi as a treatment option for PV. I encourage you to watch the other videos in the series to learn more about the management of PV.
References:
Gisslinger H. Change in polycythemia vera treatment: ropeginterferon alfa-2b in light of current trials. Turk J Haematol. 2023;40(4):266-268. doi:10.4274/tjh.galenos.2023.2023.0419
BESREMi. Prescribing information. PharmaEssentia USA Corporation; 2024.
Jayarajan J, Knoch J, Ball M, et al. Interferon-alpha treatment results in the depletion of dormant JAK2-mutant HSC in a murine model of polycythemia vera. EHA Library. 2021;324603:S195.
PharmaEssentia. PEGINVERA results. BESREMI website. Updated January 2025. Accessed March 20, 2025. https://www.besremihcp.com/peginvera-clinical-efficacy/
Data on file. PharmaEssentia Corporation.
PharmaEssentia. Safety. BESREMI website. Updated 2025. Accessed March 20, 2025. https://www.besremihcp.com/side-effects/
Barbui T, Vannucchi AM, De Stefano V, et al. Ropeginterferon versus standard therapy for low-risk patients with polycythemia vera. NEJM Evid. 2023;2(6):EVIDoa2200335. doi:10.1056/EVIDoa2200335
PharmaEssentia. Additional clinical results. BESREMI website. Updated January 2025. Accessed March 20, 2025. https://www.besremihcp.com/additional-clinical-efficacy/
Gisslinger H, Klade C, Georgiev P, et al. Ropeginterferon alfa-2b versus standard therapy for polycythaemia vera (PROUD-PV and CONTINUATION-PV): a randomised, non-inferiority, phase 3 trial and its extension study. Lancet Haematol. 2020;7(3):e196-e208. doi:10.1016/S2352-3026(19)30236-4
INDICATION
BESREMi is indicated for the treatment of adults with polycythemia vera.
IMPORTANT SAFETY INFORMATION
WARNING: RISK OF SERIOUS DISORDERS
Interferon alfa products may cause or aggravate fatal or life-threatening neuropsychiatric, autoimmune, ischemic, and infectious disorders. Patients should be monitored closely with periodic clinical and laboratory evaluations. Therapy should be withdrawn in patients with persistently severe or worsening signs or symptoms of these conditions. In many, but not all cases, these disorders resolve after stopping therapy.
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
The most common adverse reactions reported in >40% of patients were influenza-like illness, arthralgia, fatigue, pruritus, nasopharyngitis, and musculoskeletal pain.
DRUG INTERACTIONS
Patients on BESREMi who are receiving concomitant drugs which are CYP450 substrates with a narrow therapeutic index should be monitored to inform the need for dosage modification. Avoid use with myelosuppressive agents, narcotics, hypnotics, or sedatives, and monitor patients receiving the combination for effects of excessive CNS toxicity.
To report SUSPECTED ADVERSE REACTIONS, contact PharmaEssentia at 1-800-999-2449 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch
Please see full Prescribing Information, including Boxed Warning.