

FAST-CATH: A Modified Single Catheter Technique for Complete Coronary Angiography via Radial Access
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Radial access is preferred for coronary angiography because of its association with fewer vascular complications, improved patient comfort, and faster ambulation.1 Single-catheter strategies, such as using an Ikari Left 3.5 to engage both coronary arteries via right radial access, have been proposed to streamline procedures2 but remain underutilized in practice. An alternative involves a Judkins left (JL) 3.5 catheter via right radial access, with temporary insertion of a 0.035-inch stiff guidewire to reshape the curve and enable right coronary artery (RCA) engagement.3
While practical and timesaving, these techniques depend on favorable anatomy, particularly via the right radial approach. Transposition to left radial access often fails because of unfavorable angulation between the subclavian artery and aortic root. The JL 3.5 catheter frequently loses its reshaped form and coaxial alignment after removal of the stiff guidewire, often requiring exchange for a Judkins right (JR) catheter.
To address these limitations, we propose the FAST-CATH (Fast Catheterization) technique, a modified approach enabling complete coronary angiography via the left radial access or right radial in case of failure of conventional techniques, using a single 5F JL 3.5 guiding catheter and a 0.032-inch stiff guidewire introduced through a Y-connector set.
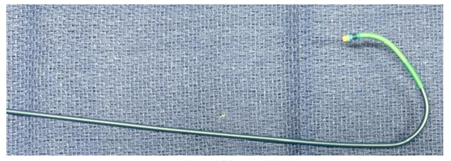
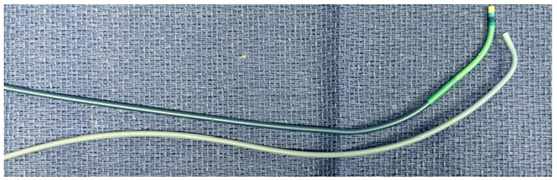
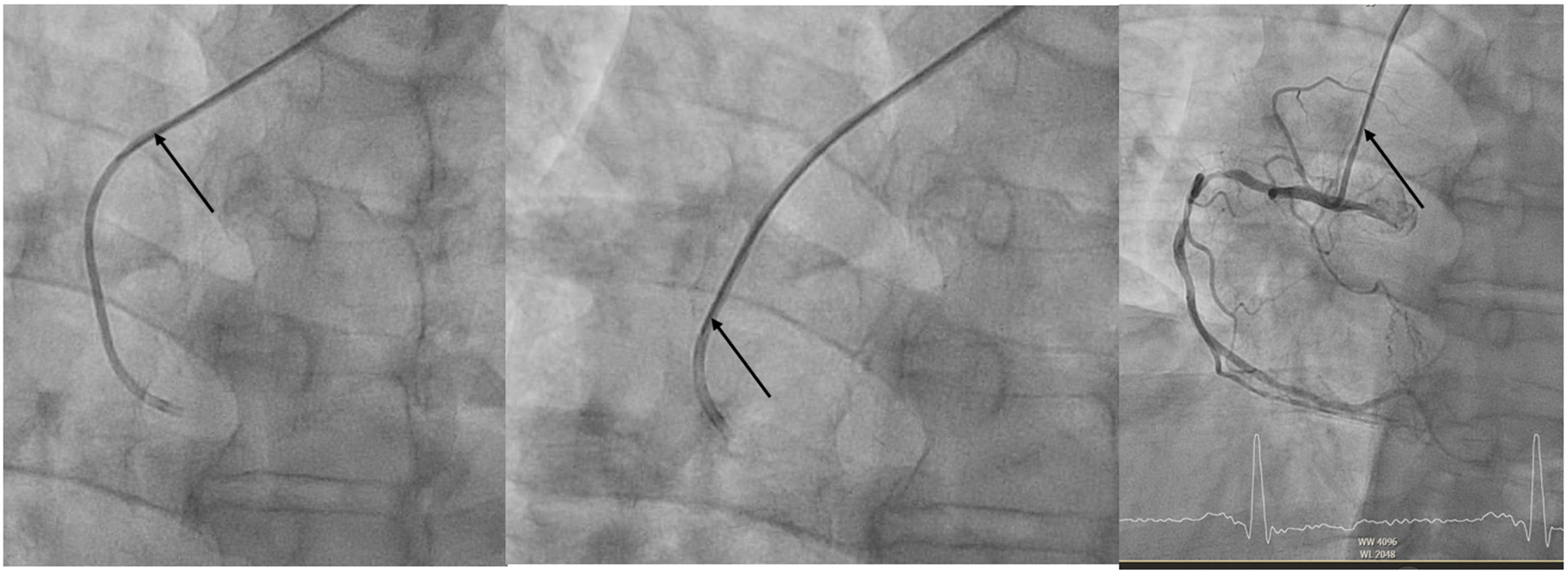
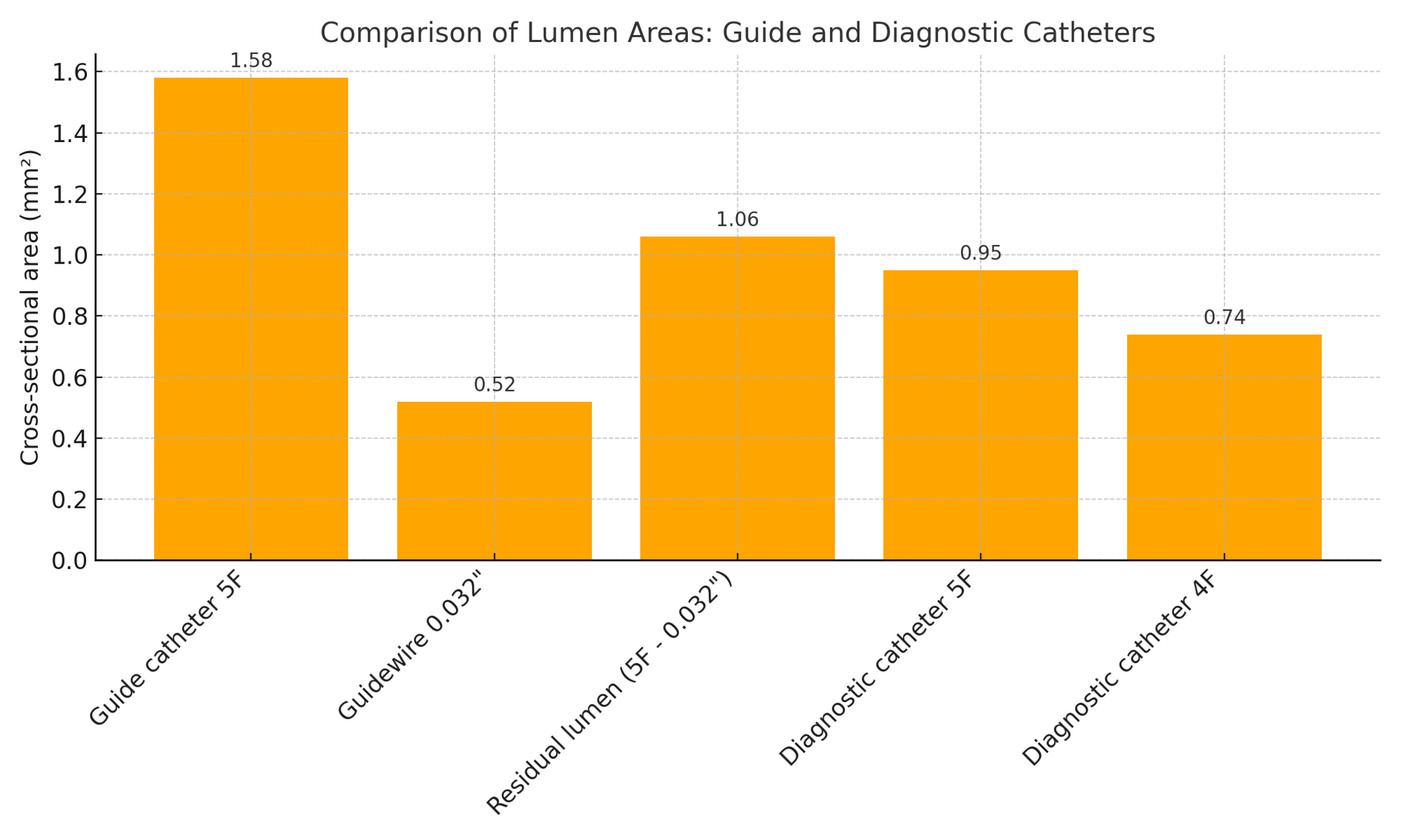
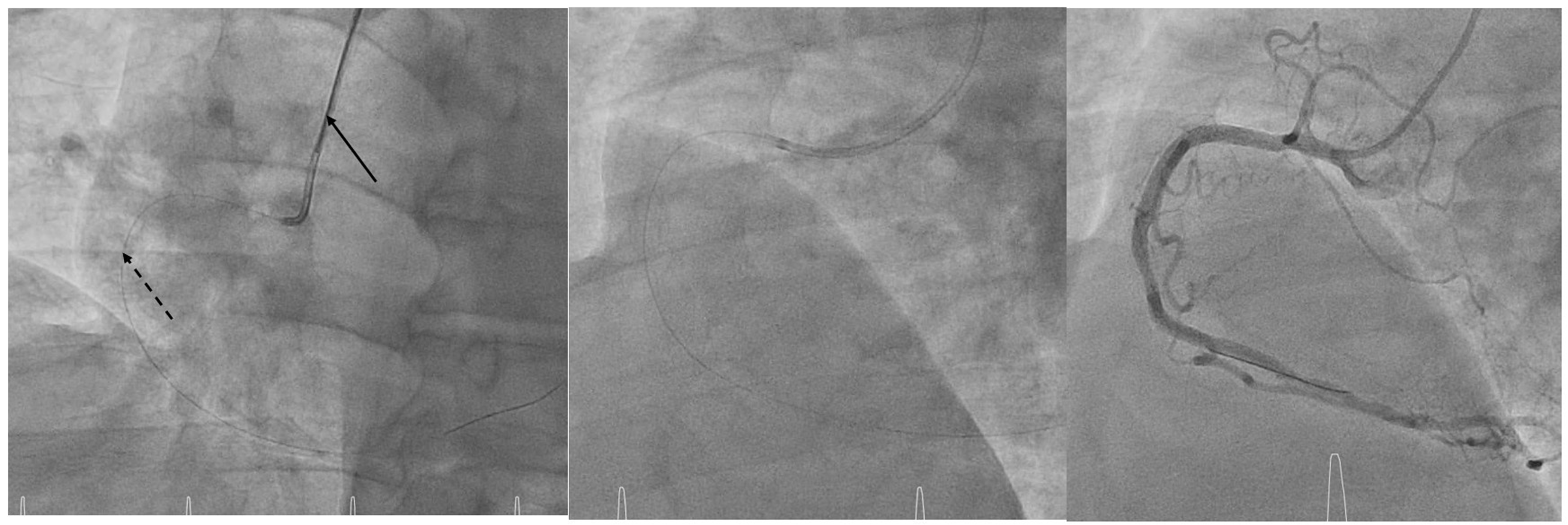
Following left coronary injections, the stiff wire is advanced so that its rigid segment extends just beyond the first curve of the catheter, straightening it into a shape mimicking a JR4 or multipurpose configuration (Figure 1). The wire is left in place during RCA injections to maintain support and coaxial alignment (Figure 2). Notably, the residual lumen of a 5F guiding catheter with a 0.032-inch wire in place (~1.06 mm²) exceeds that of a standard 5F diagnostic catheter (~0.95 mm²), ensuring safe and effective contrast delivery (Figure 3).
FAST-CATH offers several advantages: it allows complete coronary angiography with a single catheter; avoids catheter exchange; reduces procedure time, radial trauma, and spasm risk; and enables immediate transition to fractional flow reserve or ad hoc percutaneous coronary intervention (PCI). If PCI is required, a 0.014-inch wire can be advanced alongside the 0.032-inch wire, which is then withdrawn (Figure 4).
FAST-CATH provides a simple and reproducible solution for single-catheter coronary angiography via radial access; prospective validation is warranted.
Affiliations and Disclosures
Franck Digne, MD; Arthur Darmon, MD; Ludovic Maxo, MD; Victor Stratiev, MD; Mohamed Abdellaoui, MD; Mohammed Nejjari, MD
From the Cardiology Department, Centre Cardiologique du Nord, Saint Denis, France.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Franck Digne, MD, Centre Cardiologique de Nord, 32-36 Rue des Moulins Gémeaux, Saint-Denis 93200, France. Email: f.digne@ccn.fr
References
- Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79(2):e21-e129. doi:10.1016/j.jacc.2021.09.006
- Youssef AA, Hsieh YK, Cheng CI, Wu CJ. A single transradial guiding catheter for right and left coronary angiography and intervention. EuroIntervention. 2008;3(4):475-481. doi:10.4244/eijv3i4a85
- Yan Z, Xing XW, Zhang XG, Wang X, Kuang JG, Lu QH. Safety and efficacy of using Judkins left 3.5 guiding catheters for transradial right coronary artery intervention. Eur Rev Med Pharmacol Sci. 2023;27(6):2341-2349. doi:10.26355/eurrev_202303_31769










