

Leadless Pacemaker Placement Through the Subclavian Vein: An Alternative to the Femoral Route
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
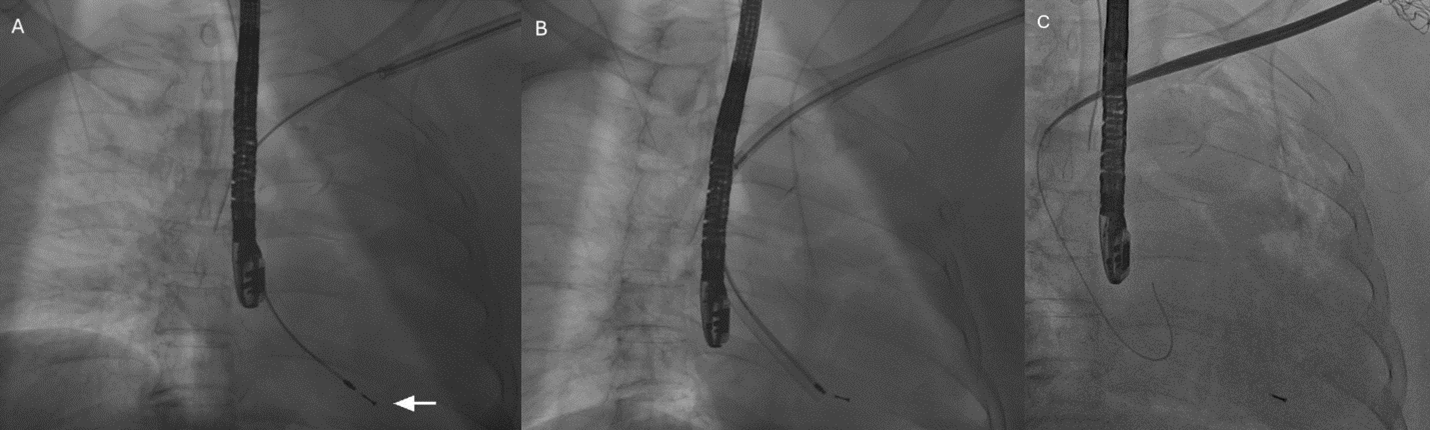
A 70-year-old woman with dementia, history of sick sinus syndrome, and permanent atrial fibrillation previously underwent dual-chamber transvenous pacemaker implantation. Over time, she developed Twiddler’s syndrome with repeated generator manipulation, resulting in diaphragmatic capture and recurrent pocket complications. The pacemaker system on the left side was extracted (Figure A-C). Intraoperative transesophageal echocardiogram was used to monitor potential lead extraction complications.
Given her recurrent pocket and lead issues, low ventricular pacing requirement, and chronic oral anticoagulation, a leadless pacemaker was selected. During the same session, an AVEIR VR Leadless Pacemaker (Abbott) was implanted via the left subclavian vein rather than the conventional femoral route. Subclavian access was selected to avoid creating new femoral access and to accommodate the patient’s request for quicker recovery, as her chronic back pain limited tolerance for prolonged bed rest.
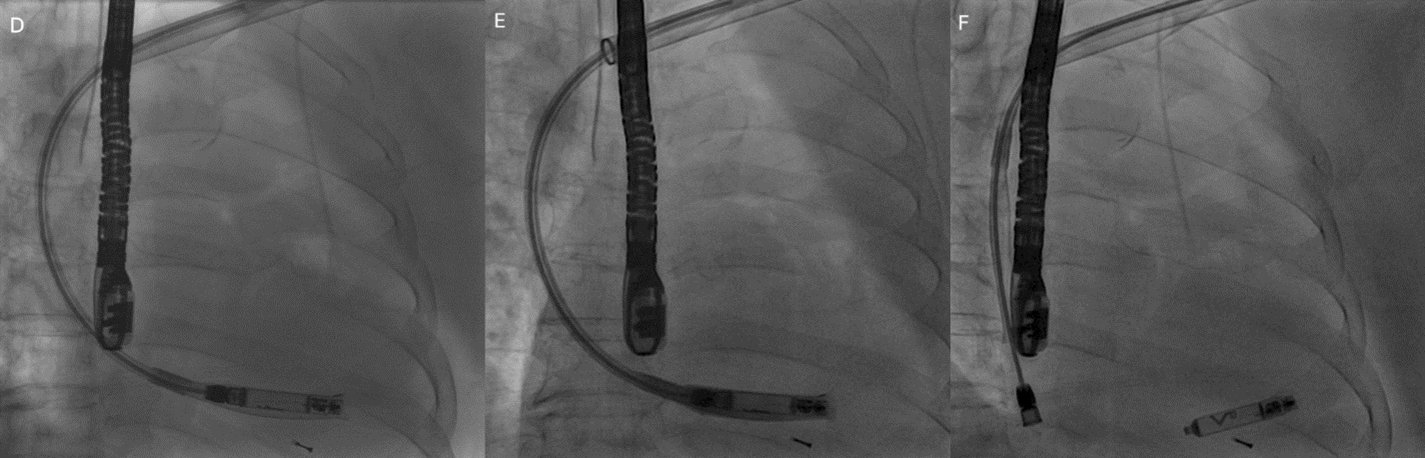
The AVEIR delivery sheath was advanced only to the distal subclavian vein to avoid vascular injury. The steerable delivery catheter was then advanced through the sheath with the protective sleeve in place and directed across the tricuspid valve into the right ventricle (Figure D and E). The device was actively fixed along the septum, and biplane fluoroscopy with contrast injection confirmed stable positioning and adequate myocardial engagement (Figure F; Videos 1-3). Electrical testing demonstrated satisfactory pacing thresholds, sensing, and impedance.
The patient tolerated the procedure without complications. At the 1- and 3-month follow-up, device interrogation confirmed stable parameters. This case highlights the feasibility of implanting a leadless pacemaker via the subclavian vein as an alternative to the standard femoral approach in select patients.
Affiliations and Disclosures
Leili Pourafkari, MD1,2; Jeong Hwan J. Kim, MD1,2; Ali Sovari, MD1,2
From the 1Cabrillo Cardiology Medical Group, Camarillo, California; 2Department of Cardiology, St. John’s Regional Medical Center, Oxnard, California.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for intervention described in the manuscript and to the publication of their data including all images. The authors report that patient consent was provided for publication of the images used herein.
Address for correspondence: Ali Sovari, MD, Department of Cardiology, St. John’s Regional Medical Center, 1600 N Rose Ave, Oxnard, CA 93030, USA. Email: alisovari@gmail.com










