

Coronary Artery Aneurysm With Thrombosis
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
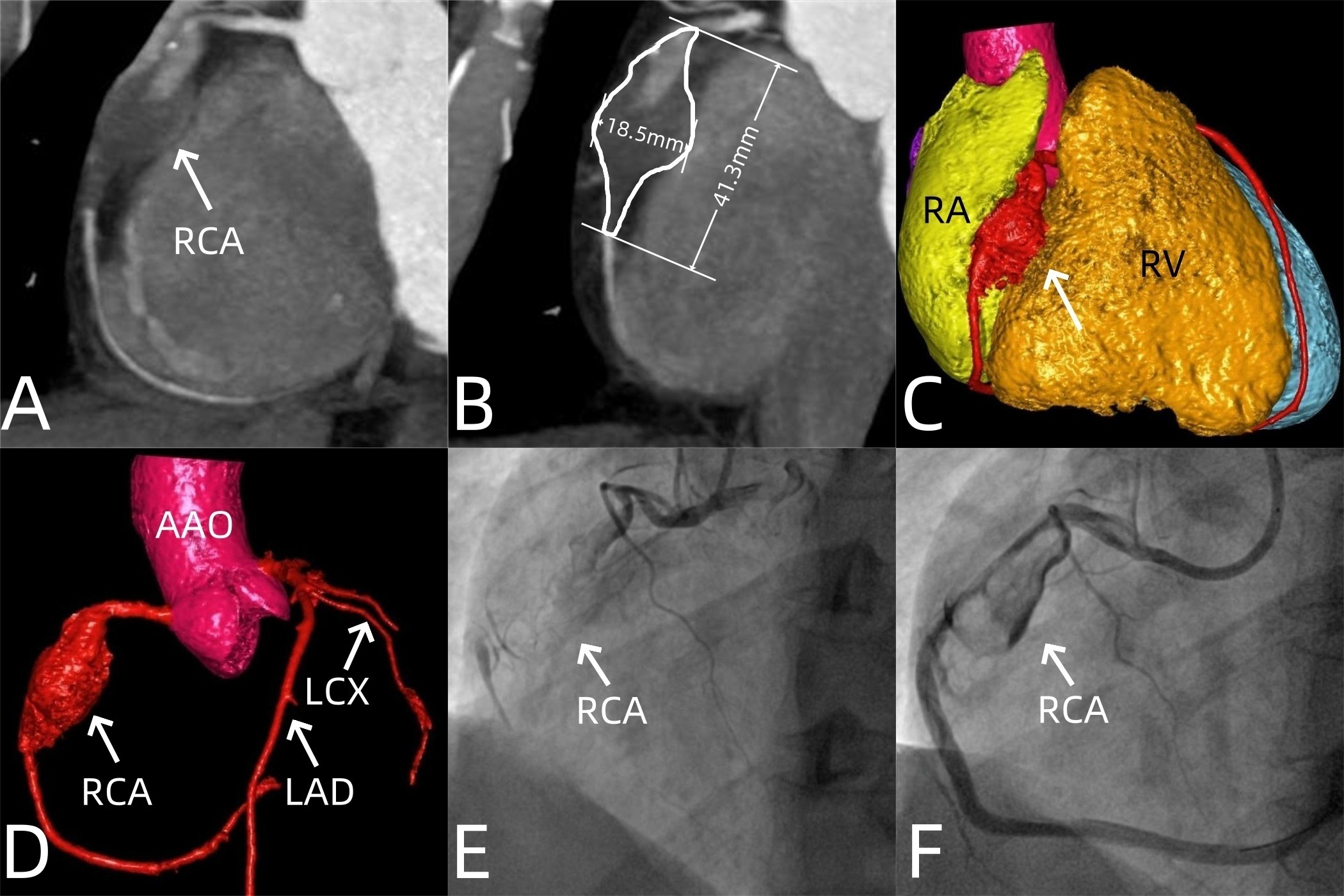
A 36-year-old man presented with chest pain lasting for half a month. Laboratory tests showed mildly elevated high-sensitivity troponin I (0.0883 ng/mL) and high-sensitivity troponin I-c (88 ng/L), along with an elevated high-sensitivity C-reactive protein (64.61 mg/L). Rheumatology-related antibodies were negative. An electrocardiogram indicated an inferior wall myocardial infarction. Coronary computed tomography angiography (CTA) revealed a fusiform aneurysm in the middle segment of the right coronary artery (RCA) (Figure). Its maximum cross-section measured 18.5 × 17.5 mm, with an affected segment length of 41.3 mm. Thrombosis was present in the aneurysm, and there were segmental occlusions in part of the aneurysm and distal lumen. Coronary angiography confirmed the CTA findings (Figure, Videos 1 and 2). After multidisciplinary team discussion, the patient underwent percutaneous transluminal coronary angioplasty with drug-coated balloon intervention in the RCA. The postoperative course was uneventful, and the patient was discharged on postoperative day 7.
Coronary artery aneurysms typically remain asymptomatic. However, complications such as intraluminal thrombosis, coronary embolism, or aneurysmal rupture often manifest with chest pain.1 Treatment modalities include medical therapy, surgical resection, coronary artery bypass grafting, and percutaneous coronary intervention.2 Cardiovascular specialists tailor treatment plans by comprehensively evaluating the aneurysm’s size, location, morphology, thrombus presence, and associated complications.
Affiliations and Disclosures
Di Huang, MD1; Xiaojing Ma, MD2; Li Zhu, MD1
From the Departments of 1Radiology and 2Echocardiography, Wuhan Asia Heart Hospital Affiliated to Wuhan University of Science and Technology, Wuhan, Hankou District, P.R. China
Dr Huang and Dr Ma served as co-first authors.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient(s) for the study and/or intervention(s) described in the manuscript and for the publication of their data.
Artificial intelligence disclosure: This manuscript was prepared without the assistance of artificial intelligence technologies, including but not limited to large language models, chatbots, or image creators.
Address for correspondence: Li Zhu, MD, Department of Radiology, Wuhan Asia Heart Hospital Affiliated to Wuhan University of Science and Technology, No.753 Jinghan Road, Hankou District, Wuhan 430022, P.R. China. Email: 476695029@qq.com
References
1. Kawsara A, Núñez Gil IJ, Alqahtani F, Moreland J, Rihal CS, Alkhouli M. Management of coronary artery aneurysms. JACC Cardiovasc Interv. 2018;11(13):1211-1223. doi:10.1016/j.jcin.2018.02.041
2. Latif A, Tran A, Ahsan J, et al. Coronary artery aneurysms as a cause of acute coronary syndrome presentation - a focused review. Curr Cardiol Rev. 2023;19(5):68-72. doi:10.2174/1573403X19666230331103508










