

Bonapace’s Branch
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
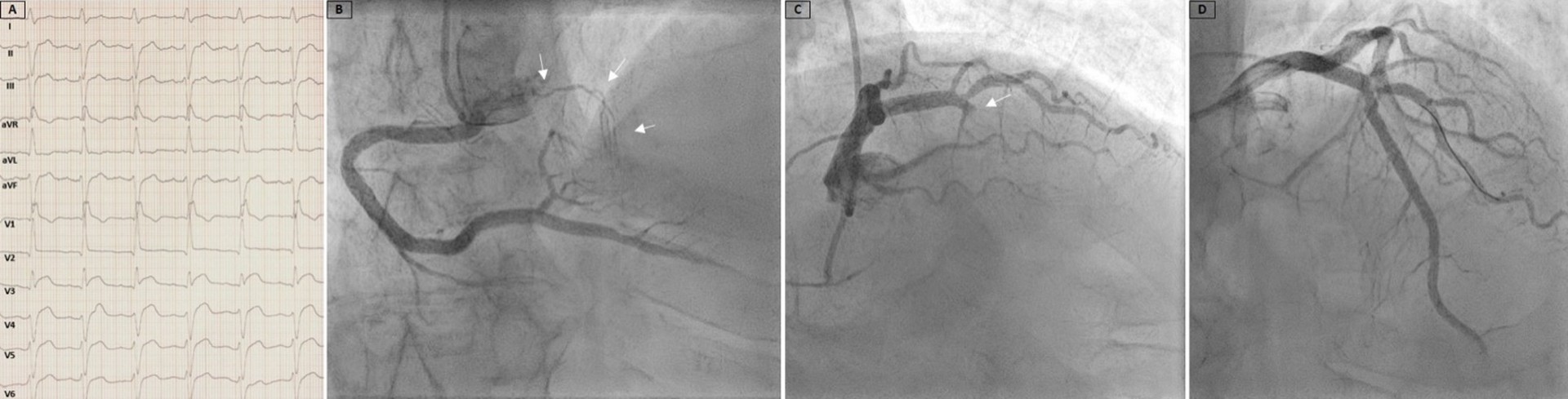
A 71-year-old man with a medical history of diabetes, hypertension, and smoking presented to the emergency department because of acute retrosternal pain. An electrocardiogram (ECG) recorded left anterior fascicular block, right bundle branch block, and ST-segment elevation in leads V3 to V5 without reciprocal changes (Figure A). Urgent coronary angiography demonstrated a descending septal artery, also known as Bonapace’s branch, arising from the proximal right coronary artery (Figure B, Video 1), and a totally occluded left anterior descending artery (LAD) in the mid-segment (Figure C, Video 2).
The occlusion was treated with implantation of a drug-eluting stent, resulting in a good angiographic result (Figure D, Video 3). The echocardiogram showed preserved ejection fraction (EF) and only moderate elevation of high-sensitivity troponin (hsTn) (hsTn-max: 9129; normal: < 34.2). The clinical course was uneventful, and the patient was discharged in good condition.
Bonapace’s branch, though an infrequent anatomical variation, provides valuable collateral circulation to the interventricular septum, atrioventricular node, and His bundle during acute or chronic occlusion of the LAD, especially in the absence of a well-developed first septal branch. In our patient, collateral blood supply through Bonapace’s branch to the acutely occluded LAD reduced the ischemic consequences, as shown by the absence of reciprocal ECG changes, moderate elevation in hsTn, and preserved EF at discharge.
Affiliations and Disclosures
Konstantinos Antoniades, MD1; Agoritsa M. Pervana, MD1; Georgios Sotiris, MD1; Ifigeneia Kiki, MD1; Christos Kostopoulos, MD1; Sotirios C. Kotoulas, MD1; Ignatios Ikonomidis, MD2; Leonidas E. Poulimenos, MD1; Andreas S. Triantafyllis, MD, PhD1
From the 1Department of Cardiology, Asklepeion General Hospital, Athens, Greece; 2Department of Cardiology, Attikon University Hospital, Athens, Greece.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient(s) for the intervention(s) described in the manuscript and for the publication thereof, including any and all images.
Address for correspondence: Konstantinos Antoniades, MD, Department of Cardiology, Asklepeion General Hospital, Leoforos Vasileos Pavlou 1, PC 16673, Voula, Athens, Greece. Email: konstantinos.a@hotmail.com










