

Suicide Left Ventricle Due to Conduction Disturbance Following Transcatheter Aortic Valve Replacement and Reversal With Restoration of Sinus Rhythm: Is There Life After Death?
Abstract: Dynamic left ventricular outflow tract obstruction and left ventricular mid-cavity obliteration are phenomena that can complicate the postoperative course in patients who undergo surgical aortic valve replacement for aortic stenosis, and may be markers of increased morbidity and mortality. Recently, reports describing dynamic intraventricular obstruction following transcatheter aortic valve replacement (TAVR) have emerged. We report a case of dynamic left ventricular mid-cavity obstruction due to disordered atrioventricular synchrony immediately following TAVR, and its reversal with restoration of atrioventricular synchrony. This case highlights the essential role of atrial contraction in the management of this phenomenon.
J INVASIVE CARDIOL 2015;27(6):E107-E109
Key words: LV mid-cavity obliteration, LVOT, transcatheter aortic valve replacement
_______________________________________
Abnormal intraventricular flow dynamics shortly after surgical aortic valve replacement (SAVR) have been described previously. It is estimated that 14% of SAVR procedures are complicated by dynamic accelerated flow velocities in the left ventricular outflow tract (LVOT), and are associated with increased morbidity and mortality.1 This phenomenon has been described following transcatheter aortic valve replacement (TAVR) and is termed “suicide left ventricle.” However, the role of atrioventricular (AV) asynchrony in the development of this complication has not been described. Although TAVR has been growing rapidly in applicability, clinical reports of pitfalls in its use are beginning to surface. We report the first description of dynamic LVOT obstruction immediately following TAVR caused by sinus arrest and AV asynchrony.
Case Report
An 81-year-old woman with symptomatic severe aortic stenosis was referred for aortic valve replacement. Significant comorbidities included non-obstructive coronary artery disease, stage III chronic kidney disease, chronic obstructive pulmonary disease, type 2 diabetes mellitus, and medically controlled hypertension. The patient was in normal sinus rhythm. Preoperative echocardiogram showed left ventricular (LV) ejection fraction of 60%-65%, mild to moderate LV 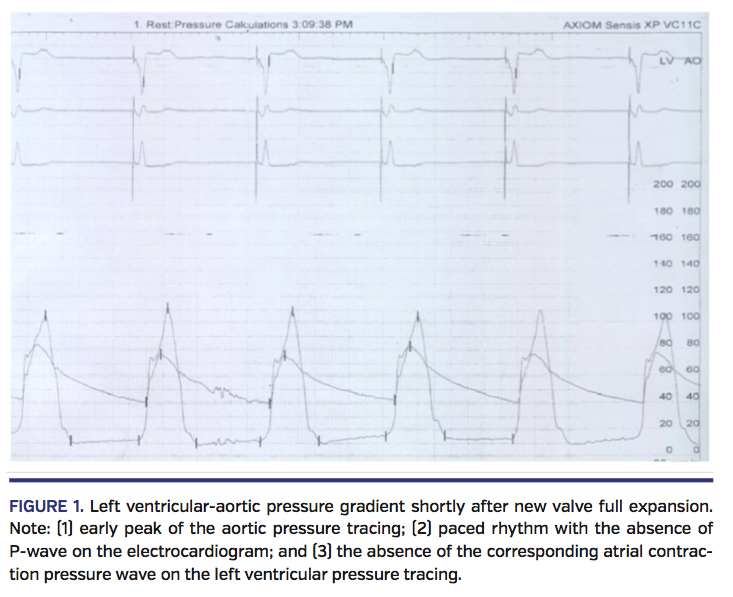 hypertrophy (interventricular septum, 1.3 cm; posterior ventricular wall, 1.5 cm), and severe aortic valve stenosis (aortic valve area, 0.42 cm2; maximum velocity, 5.23 m/s; peak gradient, 109.5 mm Hg; mean gradient, 58.6 mm Hg). There was no intracavitary or LVOT gradient. The patient underwent TAVR using the direct aortic approach through a mini sternotomy. A 29 mm CoreValve Revalving system (Medtronic) was placed at an implant depth of 4 mm. Immediately after full expansion of the new valve frame, the patient developed sinus arrest with slow escape junctional rhythm and underwent temporary right ventricular pacing. Hemodynamic assessment (Figure 1) demonstrated an LV-aortic pressure gradient with the absence of a P-wave on the electrocardiographic tracing. Mid-ventricular cavity obliteration with LVOT flow acceleration was also noted on accompanying transesophageal echocardiogram (Figure 2; Videos 1 and 2). Within 42 seconds, spontaneous restoration of atrial electrical activity occurred with subsequent resolution of the LV-aortic pressure gradient without any medical or procedural intervention (Figure 3; Video 3).
hypertrophy (interventricular septum, 1.3 cm; posterior ventricular wall, 1.5 cm), and severe aortic valve stenosis (aortic valve area, 0.42 cm2; maximum velocity, 5.23 m/s; peak gradient, 109.5 mm Hg; mean gradient, 58.6 mm Hg). There was no intracavitary or LVOT gradient. The patient underwent TAVR using the direct aortic approach through a mini sternotomy. A 29 mm CoreValve Revalving system (Medtronic) was placed at an implant depth of 4 mm. Immediately after full expansion of the new valve frame, the patient developed sinus arrest with slow escape junctional rhythm and underwent temporary right ventricular pacing. Hemodynamic assessment (Figure 1) demonstrated an LV-aortic pressure gradient with the absence of a P-wave on the electrocardiographic tracing. Mid-ventricular cavity obliteration with LVOT flow acceleration was also noted on accompanying transesophageal echocardiogram (Figure 2; Videos 1 and 2). Within 42 seconds, spontaneous restoration of atrial electrical activity occurred with subsequent resolution of the LV-aortic pressure gradient without any medical or procedural intervention (Figure 3; Video 3).
Discussion
To the best of our knowledge, this is the first report of the role of AV synchrony in modulating intraventricular cavity obliteration and increased flow velocity following TAVR. This case demonstrates the importance of maintaining atrial contraction (thus maximizing LV filling) to avoid such a complication.
LV cavity obliteration following TAVR has been attributed to infundibular hypertrophy and hypercontractility following the relief of longstanding fixed obstruction.2 Given its similarity to the physiology of suicide right ventricle after successful pulmonic valvuloplasty, this phenomenon was termed suicide LV.2,3 Management is focused on maintaining normal — or in some cases supranormal — LV filling pressures, decreasing chronotropy, and minimizing inotropy to relieve the obstruction. Emergency alcohol septal ablation during the procedure has also been described in refractory cases, particularly to relieve obstruction caused by systolic anterior motion of the anterior mitral leaflet.4 As demonstrated in our case, AV synchrony plays an essential role in the early management of suicide LV following TAVR.
Increased intraventricular flow velocity and LVOT obstruction following SAVR have been previously described. Although the mechanism is still poorly understood, inotropic stimulants, volume depletion, and peripheral vasodilation can  exacerbate LVOT obstruction.1 Echocardiographic predictive factors for the development of this phenomenon include small LV end-diastolic diameter, supranormal ejection fraction, and high baseline valve gradient. The development of AV block resulting in underfilling of a hypertrophied and non-compliant LV is usually underrecognized. Institution of dual-chamber pacing has resulted in resolution of the ventricular-aortic pressure gradient following SAVR.5 The most plausible explanation for our observation in this case is the loss of atrial contraction resulting in loss of preload in a non-compliant LV, accompanied by the sudden decrease in impedance to LV ejection.
exacerbate LVOT obstruction.1 Echocardiographic predictive factors for the development of this phenomenon include small LV end-diastolic diameter, supranormal ejection fraction, and high baseline valve gradient. The development of AV block resulting in underfilling of a hypertrophied and non-compliant LV is usually underrecognized. Institution of dual-chamber pacing has resulted in resolution of the ventricular-aortic pressure gradient following SAVR.5 The most plausible explanation for our observation in this case is the loss of atrial contraction resulting in loss of preload in a non-compliant LV, accompanied by the sudden decrease in impedance to LV ejection.
Conduction disturbances are well described following both SAVR and TAVR, with an estimation of 5%-8% for SAVR and as many as 30% of patients in some series of TAVR. Heart block, the most common form of conduction dysfunction in the setting of TAVR, generally occurs shortly after either preparatory balloon valvuloplasty or full expansion of the new aortic valve frame. Sinus arrest and/or severe sinus bradycardia can rarely complicate the procedure; in one study, the incidence of severe bradycardia requiring permanent pacemaker implantation after TAVR was 1.7%.6 Often, the observed conduction dysfunction is transient. In the acute setting, single-chamber (usually right ventricle) pacing through an intravenous temporary pacer wire is the option to restore the heart rate. The presence of factors that may increase the likelihood of AV block (preoperative right bundle branch block, increased implant depth, and valve oversizing) should alert the implanting team to the possible development of dynamic LV cavity obliteration following implantation. Furthermore, access to dual-chamber pacemaker should be readily available is such cases.
Conclusion
In the presence of an unexplained ventricular to aortic gradient after successful valve implantation, dynamic LVOT obstruction as a consequence of conduction abnormalities (ie, AV dissociation and/or sinus arrest) should be considered and  preparations for synchronized dual-chamber AV pacing should be made, along with the routine management with fluid resuscitation and beta-blockers. The current case highlights the role of atrial contraction in augmenting LV preload during and shortly after TAVR.
preparations for synchronized dual-chamber AV pacing should be made, along with the routine management with fluid resuscitation and beta-blockers. The current case highlights the role of atrial contraction in augmenting LV preload during and shortly after TAVR.
References
- Bartunek J, Sys SU, Rodrigues AC, et al. Abnormal systolic intraventricular flow velocities after valve replacement for aortic stenosis mechanisms, predictive factors, and prognostic significance. Circulation. 1996;93:712-719.
- Suh WM, Witzke CF, Palacios IF. Suicide left ventricle following transcatheter aortic valve implantation. Catheter Cardiovasc Interv. 2010;76:616-620.
- Ben-Shachar G, Cohen MH, Sivakoff MC, et al. Development of infundibular obstruction after percutaneous pulmonary balloon valvuloplasty. J Am Coll Cardiol. 1985;5:754-756.
- Krishnaswamy A, Tuzcu EM, Svensson LG, Kapadia SR. Combined transcatheter aortic valve replacement and emergent alcohol septal ablation. Circulation. 2013;128:e366-e368.
- Ishaq M, Pacing to treat low cardiac output syndrome following elective aortic valve replacement. Saudi J Anaesth. 2012;6:169-171.
- Bagur R, Rodes-Cabau J, Gurvitch R, et al. Need for permanent pacemaker as a complication of transcatheter aortic valve implantation and surgical aortic valve replacement in elderly patients with severe aortic stenosis and similar baseline electrocardiographic findings. JACC Cardiovasc Interv. 2012;5:540-551.
__________________________________________
From Houston Methodist DeBakey Heart & Vascular Center, Houston, Texas; and Weill Cornell Medical College, New York, New York.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted June 4, 2014, provisional acceptance given July 14, 2014, final version accepted September 17, 2014
Address for correspondence: Neal S. Kleiman, MD, 6565 Fannin, MS F10-035, Houston, TX 77030. Email: nkleiman@houstonmethodist.org










