


Total Talus Replacement with Polyetherketoneketone (PEKK) Implant: A Novel Solution for Complex Ankle Pathology
Total talus replacement is emerging as a powerful salvage option for patients with advanced avascular necrosis (AVN), failed ankle arthroplasty, or end-stage ankle arthritis. This article explores the advantages of 3D-printed polyetherketoneketone (PEKK) implants over traditional metallic talar prostheses, including reduced risk of metallosis, improved biomechanical compatibility, and enhanced imaging capabilities. A complex revision case highlights the clinical application and early functional outcomes of PEKK total talus replacement.
Key Takeaways
1. PEKK Offers Biomechanical and Biological Advantages Over Metal Implants. Unlike titanium, PEKK more closely matches the stiffness of native bone, reducing stress shielding and potential damage to adjacent articular surfaces. It is radiolucent, customizable through 3D printing, and demonstrates inherent antibacterial properties.
2. Metallic Talar Implants Carry Documented Risks. Metal implants may lead to metallosis, hypersensitivity reactions, elevated systemic metal levels, and adjacent cartilage damage. These complications can complicate revision surgery and may mimic infection clinically.
3. PEKK Total Talus Replacement Is a Promising Salvage Option in Complex Cases. In revision settings, particularly after failed metallic implants, 3D-printed PEKK talar prostheses can restore alignment, improve range of motion, and avoid metal-related complications. While early outcomes are encouraging, long-term survivorship data are still needed.
Talar pathologies are complex, ranging from talus collapse to end-stage degeneration, and most often result from avascular necrosis (AVN) or advanced arthritis. These conditions remain a challenge in foot and ankle surgery. Standard treatment like arthrodesis can restore stability but often sacrifices motion. Metallic talar implants, once considered a salvage option, bring their own challenges, including metallosis, hypersensitivity and damage to adjacent articular surfaces. As recognition grows for the need for salvage solutions, particularly after failed ankle arthroplasty, total talus replacement with polyetherketoneketone (PEKK) has emerged as a potential solution. This article introduces PEKK implants for total talus replacement, contrasts them with titanium implants, and highlights a revision case example to display their clinical application.

Talus Anatomy and Biomechanics
The talus is a critical bone in hindfoot biomechanics, bearing body weight while articulating with the tibia, fibula, calcaneus, and navicular. Because of its limited blood supply, the talus is particularly vulnerable to AVN. The majority of the talus surface is covered by articular cartilage, leaving minimal space for vascular supply and increasing risk of AVN and degeneration. Unlike other foot bones, the talus has no tendinous attachments, relying only on its ligamentous structures for stability. Functionally, the talus is key for ankle dorsiflexion/plantarflexion and subtalar inversion/eversion. The talus, being the central bone articulating with multiple joints in the hindfoot, plays a critical role in normal gait mechanics. These unique anatomic and vascular features make it especially challenging when collapse or degeneration occurs.
Challenges with Metallic Implants
Metallic talar implants are used widely, however they have several important challenges. First, metallosis can occur as wear debris accumulates. Over time, the wear of metallic implants can release metal debris, leading to metallosis with pain, inflammation, and tissue destruction.1 Eventually, this can lead to osteolysis or erosion and can affect adjacent articular surfaces. Dapunt and colleagues describe how metallosis in hip arthroplasty can mimic infection, presenting with overlapping symptoms such as pain and elevated inflammatory markers.2 Although this work focused on the hip, the same diagnostic challenge applies to the ankle when using metallic implants. While ankle-specific research remains limited, Tandon and team noted in their review of hip and knee arthroplasty that cobalt and chromium debris from implant wear and corrosion can lead to local pain, tissue destruction, and systemic complications ranging from cardiomyopathy to neuropsychiatric symptoms.1
Second, metallic hypersensitivity poses another risk. Hallab and coworkers estimated that up to 15% of the United States’ population may have metal sensitivity.3 Haston and colleagues discussed a case report regarding a patient that developed diffuse rash 7 weeks after a total ankle arthroplasty.4 This patient ultimately tested positive for metal allergy and converted to an ankle arthrodesis. This case shows that metal allergies can significantly complicate the decision for ankle replacement, potentially leading to restricted ankle motion.
Finally, systemic exposure remains a concern with metal implants. In a retrospective study, Cohen and team observed elevated serum titanium levels in patients with ankle arthroplasty.5 Such findings emphasize the potential systemic absorption of implant debris. Rakow and coworkers demonstrated that serum neurofilament light levels closely mirrored cerebrospinal fluid (CSF) concentrations—patients showed median of 73 pg/mL in serum versus 2,418 pg/mL in CSF compared with 1pg/mL and 533 pg/mL in controls, respectively.6 This confirms that serum levels can serve as a reliable, noninvasive biomarker testing.5
PEKK as an Alternative to Metal Implants
PEKK (polyetherketoneketone) implants provide alternatives to metal implants for ankle arthroplasty. Their advantages can be grouped into mechanical, biological and clinical handling categories. PEKK’s stiffness is more closely related to bone compared to titanium. With mechanical properties closer to bone, PEKK distributes load more evenly and reduces stress shielding. By contrast, in the study by Haston and colleagues, they found metallic pitting in more than half of tibial components and nearly all talar components on microscopic analysis.4
Due to its lower stiffness and smoother characteristics, PEKK is less likely to damage adjacent articular surfaces and produce wear debris. Alqurashi and team describe how this lower stiffness helps preserve adjacent articular surfaces, an important consideration given that titanium can damage opposing cartilage and bone.6

Unlike metal, PEKK is radiolucent, allowing for more accurate intraoperative and postoperative imaging. This material can also be 3D-printed, making it compatible with patient specific implant needs, particularly in complex revision cases.
PEKK demonstrates inherent antibacterial properties, which provide strong bacterial resistance without using additional antibiotics as coverage postoperatively. Wang and colleagues also showed that nanostructured PEKK surfaces significantly reduced bacterial attachment (by 37% for Staphylococcus epidermidis and up to 50% for Pseudomonas aeruginosa compared to standard polyether-ether ketone (PEEK)) without antibiotics.7

A Closer Look at a Representative Case
A 60-year-old male with a history of hypertension, hyperlipidemia, and prior total talus replacement with a metallic talar implant for end-stage ankle osteoarthritis presented with persistent ankle pain and stiffness. He reported progressive symptoms that significantly limited his activities of daily living. He reduced his walking tolerance, could not stand for prolonged periods, and had difficulty ascending and descending stairs. On physical examination, he demonstrated no appreciable edema, but crepitus occurred with ankle motion. He exhibited limited range of motion, with dorsiflexion from 0–3 degrees and plantarflexion to 45 degrees, and he reported pain at end range. Palpation elicited circumferential tenderness around the ankle joint, particularly within the medial and lateral gutters. Gait evaluation reproduced pain and revealed an antalgic pattern. Despite undergoing total talus replacement, he continued to experience pain with range of motion and ongoing functional limitation. Advanced imaging revealed areas of impingement and cystic formation surrounding the implant that likely contributed to his persistent pain and stiffness, which ultimately led us to consider revision surgical intervention. He elected for revision of the total talus replacement with PEKK implant, internal brace, and biocartilage augmentation.
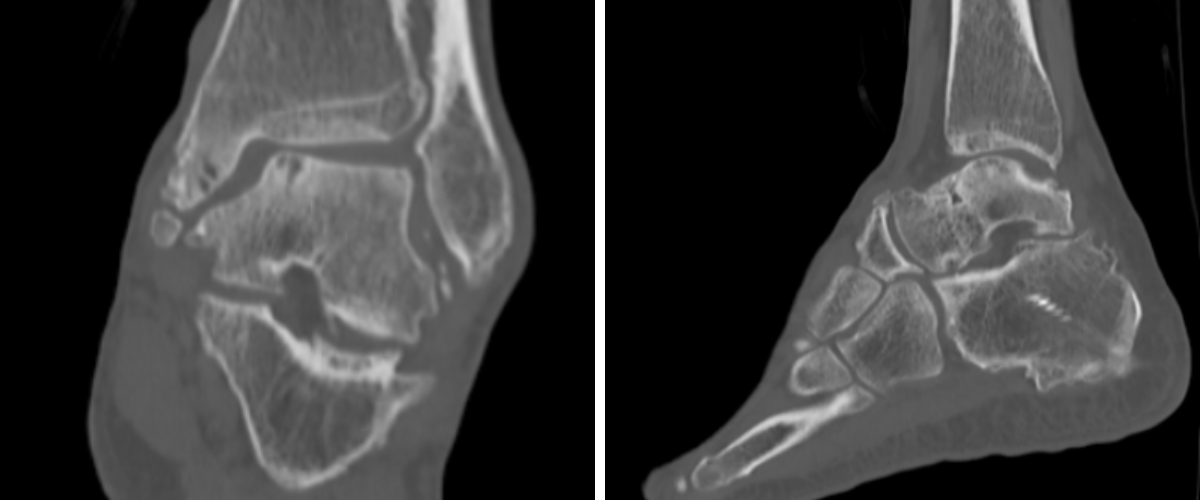
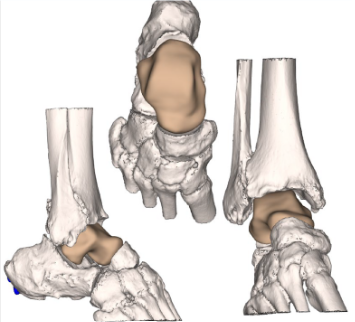
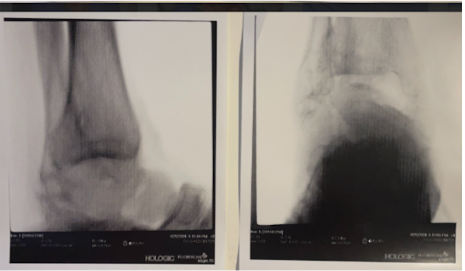
Preoperative plain film imaging demonstrated intact hardware with slight lateral deviation, implant tilt, medial tibiotalar joint space narrowing, varus deformity, and degenerative changes in both the tibiotalar and subtalar joints (Figure 1). Computed tomography (CT) confirmed subchondral sclerosis and erosive changes along the tibial plafond and subtalar articular surface (Figure 2). In addition, CT imaging of the contralateral ankle guided preoperative planning and informed patient-specific implant design. A 3D model with prototype images assisted with preoperative planning (Figure 3). The final implant was manufactured from 3D-printed PEKK by Oxford Performance Materials (OPM).

In the operating room, we made a linear anterior incision over the ankle, dissected through subcutaneous tissue and carefully retracted the anterior tibial tendon and neurovascular structures. We carried dissection down until visualizing the talus. Then, we performed a transverse coronal osteotomy through the talar neck, which we then resected. The sagittal osteotomy bisected the talar body and we removed the halves. Inspection of the surrounding soft tissue revealed metallic debris consistent with metallosis reaction (Figure 4). We sent an intraarticular culture which eventually revealed no organism growth. The calcaneus and tibial plafond also exhibited cartilage erosion, for which we used biocartilage augmentation. Next, we initiated trial implant sizing using the nominal-sized trial based on preoperative templating. We inserted the trial into the prepared site, and evaluated its position in relation to the tibial plafond, calcaneus, and navicular. Using a power drill, we installed an Arthrex InternalBrace onto the lateral talar process of the nominal 3D talus implant (Figure 5). After placing the implant into the ankle joint, we sutured the InternalBrace into the scarred anterior talofibular ligament remnant laterally (Figure 6). The implant demonstrated congruent articulation and cortical support without overhang or impingement. Ankle range of motion assessment intraoperatively demonstrated smooth dorsiflexion and plantarflexion. Intraoperative fluoroscopy confirmed adequate positioning and alignment of the implant (Figure 7).
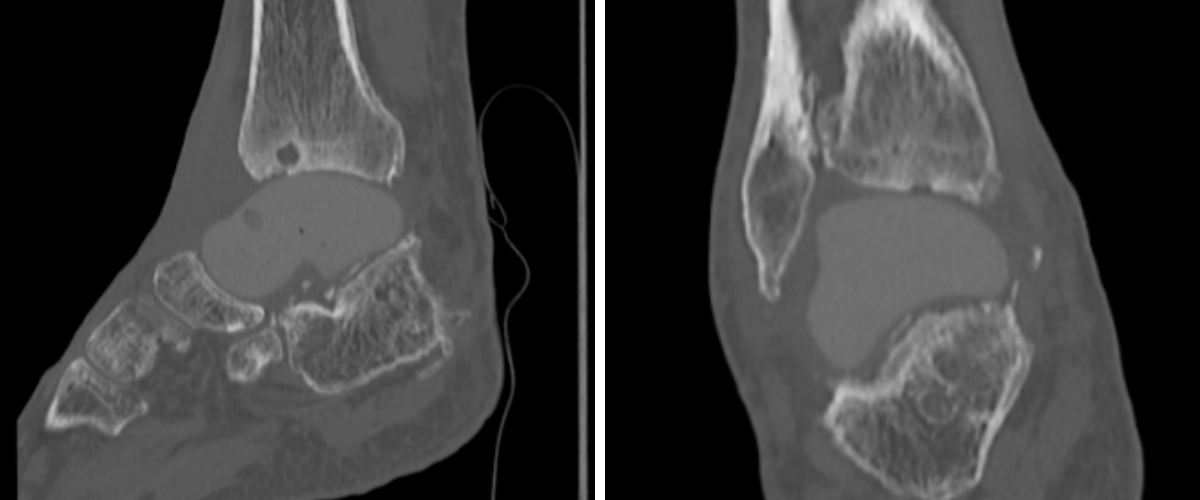
Postoperatively, radiographs and CT scans confirm proper alignment of the PEKK implant without any varus malalignment and adequate positioning (Figures 8 and 9). Postoperative ankle range of motion improved to 5 degrees dorsiflexion and 55 degrees plantarflexion. The patient remained non-weight-bearing for 3 weeks in a cast boot. He progressed to weight-bearing as tolerated in ankle stirrup brace with physical therapy. He returned to full activity and work by 6 months postoperative.
This revision restored ankle alignment and stability while avoiding the metallic debris–related complications seen with his prior implant, highlighting the utility of PEKK implants in complex revision total talus replacement cases.

Future Directions
Further research is needed to better define the role of PEKK talar implants. Long-term outcome studies and multicenter registries will help clarify survivorship and complication rates. Standardized surgical technique training and education will be essential. Continued research into biologic integration, antimicrobial surface design, and cost-effectiveness will also guide the future of this technology. Some limitations in using custom implants are the cost of these implants, the learning curve for surgeons, and limited long-term outcome data. Current clinical applications for PEKK total talus replacement include complex revision cases, advanced AVN, and severe ankle arthritis where other treatment options are limited.
Conclusions
Total talus replacement with PEKK implants represents a promising step forward in managing complex ankle pathology. Compared to titanium, PEKK offers distinct advantages: biocompatibility, radiolucency, reduced risk of metallosis, preservation of adjacent articular surfaces, and even antimicrobial potential. While early outcomes are encouraging, further research and collaboration will be necessary to establish long-term success and to develop standardized surgical protocols. As technology evolves, PEKK may expand the reconstructive options available for patients with end-stage talar degeneration.
Dr. Krishnan is a third-year podiatric surgery resident at the Department of Veterans Affairs, Palo Alto Health Care Systems in Palo Alto, CA.
Dr. Kaur is a second-year podiatric surgery resident at the Department of Veterans Affairs, Palo Alto Health Care Systems in Palo Alto, CA.
Dr. Warne is Section Chief of the Department of Podiatric Surgery, Department of Surgery at the Department of Veterans Affairs, Palo Alto Health Care Systems in Palo Alto, CA.
References
1. Tandon M, Chetla N, Hodges J, et al. Mechanical considerations and clinical implications of joint arthroplasty metallosis. Cureus. 2024;16(12):e76592. doi:10.7759/cureus.76592
2. Dapunt U, Giese T, Lasitschka F, Reinders J, Lehner B, Kretzer JP, Ewerbeck V, Hänsch GM. On the inflammatory response in metal-on-metal implants. J Transl Med. 2014;12:74. doi:10.1186/1479-5876-12-74
3. Hallab NJ, Jacobs JJ. Biologic effects of implant debris. Bull NYU Hosp Jt Dis. 2009;67(2):182-188.
4. Haston S, Langton D, Townshend D, Bhalekar R, Joyce T. Metal debris release is commonly seen from explanted total ankle replacements. J Mech Behav Biomed Mater. 2023;144:105932. doi:10.1016/j.jmbbm.2023.105932
5. Cohen WB, Hur ES, Quigley L, Skipor AK, Lin JL, Lee S, Jacobs JJ, Bohl DD. Serum metal levels following total ankle arthroplasty. Foot Ankle Orthop. 2024;9(4):2473011424S00494. doi:10.1177/2473011424S00494
6. Alqurashi H, Khurshid Z, Syed AUY, Rashid Habib S, Rokaya D, Zafar MS. Polyetherketoneketone (PEKK): an emerging biomaterial for oral implants and dental prostheses. J Adv Res. 2020;28:87-95. doi:10.1016/j.jare.2020.09.004
7. Wang M, Bhardwaj G, Webster TJ. Antibacterial properties of PEKK for orthopedic applications. Int J Nanomedicine. 2017;12:6471-6476. doi:10.2147/IJN.S134983
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.





