


Absolute and Relative Contraindications for Total Ankle Replacement: A Practical Guide
Understanding absolute and relative contraindications to total ankle replacement helps surgeons minimize complications such as loosening, wound failure, and early revision. This article provides a practical, evidence-informed framework to guide clinical decision-making in modern ankle arthroplasty.
Key Takeaways
- Not all contraindications are equal. Absolute contraindications—such as active infection, severe peripheral vascular disease, Charcot neuroarthropathy, and uncorrectable deformity—generally preclude total ankle replacement, while relative contraindications may be addressed with careful optimization and surgical planning.
- Alignment, bone quality, and soft tissue health are foundational. Successful TAR depends on correctable deformity, sufficient bone stock, ligamentous stability, and a healthy soft tissue envelope to reduce the risk of implant failure and wound complications.
- Modern TAR demands individualized risk stratification. Advances in implant design and surgical technique have expanded candidacy, but surgeons must balance patient age, activity level, comorbidities, and long-term revision risk when choosing between ankle replacement and arthrodesis.
Determining who should not undergo total ankle replacement (TAR) is as important as knowing who should. Contraindications, both absolute and relative, are crucial in minimizing complications such as implant loosening, infection, and early failure. This article reviews the most widely accepted contraindications to TAR, discusses the reasoning behind each, and offers practical guidance for surgeons evaluating for and performing this procedure.
The ankle is a complex, load-bearing joint that operates under tremendous stress over a relatively small surface area.1 Successful TAR requires balanced alignment, solid bone stock, stable ligaments, and healthy soft tissue coverage. Insufficiency in any of these areas increases the risk of early implant failure.2
Preoperative assessment should therefore include a thorough review of the patient’s overall health, vascular, and neurologic statuses, soft tissue envelope and ligamentous stability, bone quality, and deformity characteristics. Many contraindications arise from deficiencies in these categories.
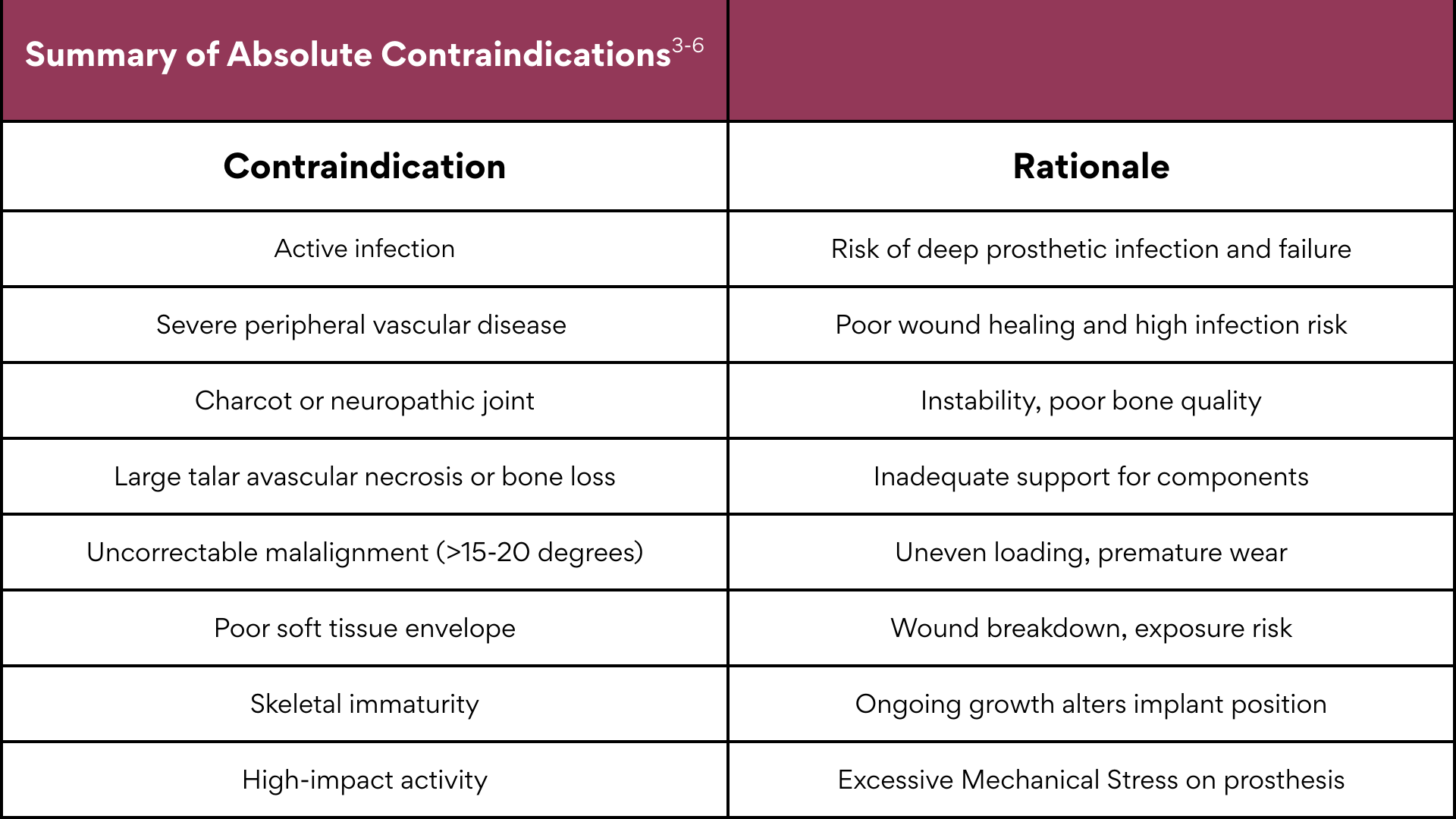
Absolute Contraindications
Absolute contraindications are those in which TAR is generally not advised under any circumstance, as the risk of total failure outweighs any potential benefit.
Active or Recent Infection. Whether in the joint, bone, overlying soft tissue, or elsewhere, infection poses an unacceptable risk for prosthetic contamination and failure. Even remote infections such as abdominal wounds or infected ingrown toenails should delay total ankle replacement. Moreover, history of osteomyelitis of the tibia or talus, or a septic ankle joint, require culture and biopsy to rule out chronic infection before proceeding with TAR.
Severe Peripheral Vascular Disease. Adequate blood flow is essential for wound healing and osseointegration. Patients with critical limb ischemia, absent pulses, or significantly diminished perfusion are poor candidates for TAR. Without sufficient vascular supply, wound complications and deep infection rates rise sharply.3 If there is a question of a patient's vascular supply to the lower extremity it is wise to order noninvasive vascular tests. In our experience, patients with vascular disease are typically better served by conservative management of their ankle arthritis.
Neuropathic (Charcot) Arthropathy. Loss of protective sensation and joint proprioception, as seen in diabetic Charcot neuroarthropathy, creates a highly unstable mechanical environment. Poor bone quality, and the hypothetical risk of causing an acute Charcot event cause these patients to be poor candidates for a total ankle replacement. In such cases, ankle fusion may provide better long-term stability and function.4
Extensive Avascular Necrosis or Severe Bone Loss. The talus is the foundation for the prosthesis and bone quantity is limited. When avascular necrosis involves more than roughly one-third of the talar body, there is insufficient support for the talar component.5 Likewise, extensive tibial or talar bone loss, whether from trauma, cystic change, or prior surgery, prevents reliable fixation. Management of these scenarios is often best with fusion or custom total talus reconstruction instead.
Uncorrectable Deformity. A TAR relies on even load distribution across the implant. If coronal or sagittal plane deformity exceeds approximately 15-20 degrees and one cannot correct this surgically, the risk of eccentric loading and premature wear rises dramatically.6,7 Halai and colleagues found that there are similar failure rates of total ankle replacement for patients that have greater than 15 degrees of deformity compared to those with less than that level, as long as the deformity is corrected.6 If deformity correction is not possible, then the patient is not a candidate for total ankle replacement
Inadequate Soft Tissue or Neuromuscular Control. In our experience, stable, well-perfused soft-tissue envelope is vital for wound healing. Severe scarring, previous radiation, or chronic steroid use may render the skin too fragile to tolerate surgical exposure. Additionally, patients with significant neuromuscular disorders or paralysis lack the muscle control needed for postoperative gait stability, making TAR a poor option.
Skeletal Immaturity. Because prostheses are designed for mature bone anatomy, TAR is contraindicated in patients with open growth plates or skeletal immaturity.
High-Impact Occupation or Lifestyle. Patients engaged in heavy labor, contact sports, or other high-impact activities are poor candidates. Repetitive jumping, running, or carrying heavy loads accelerates component wear and loosening. Although this criterion is somewhat surgeon-dependent, in most community settings, surgeons treat this as an absolute exclusion.
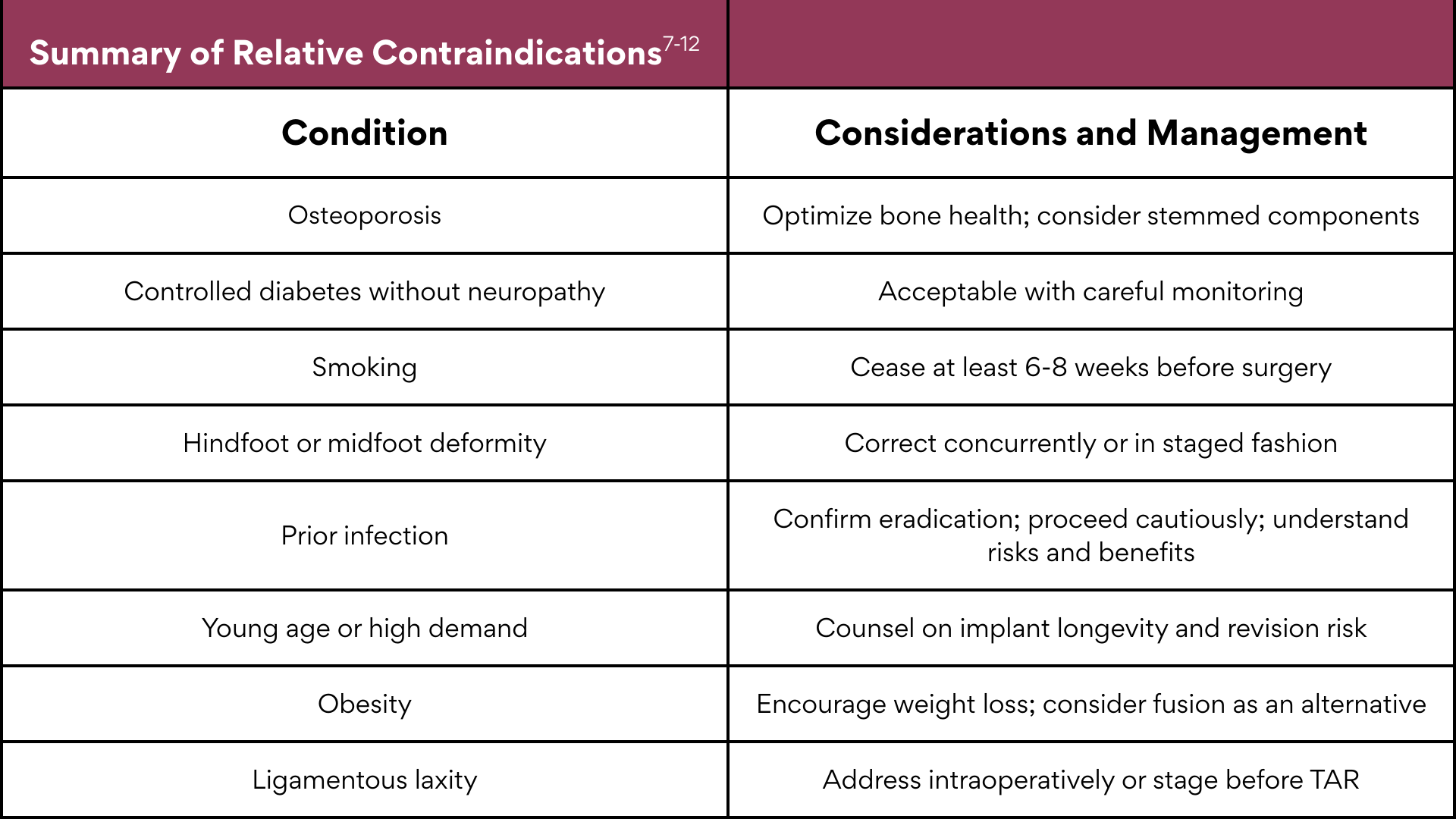
Relative Contraindications
Relative contraindications do not automatically preclude TAR but signal increased risk. With appropriate optimization, some patients in this group may still be suitable candidates.
Osteoporosis or Poor Bone Quality.4 Reduced bone density compromises implant fixation and stability. Patients with advanced osteoporosis are hypothetically more prone to subsidence and loosening. Surgeons should assess bone health preoperatively and address modifiable factors such as vitamin D deficiency or steroid use prior to surgery.
Diabetes Mellitus and Peripheral Neuropathy. Patients with diabetes, good glycemic control, and intact sensation can do well with TAR. However, poorly controlled diabetes and any degree of sensory neuropathy significantly increase the risk of infection and wound complications.4 Neuropathy remains one of the most debated relative contraindications; while mild cases may be acceptable, profound sensory loss or Charcot changes remain disqualifying.
Smoking and Other Modifiable Risks. Nicotine impairs blood flow and inhibits wound healing. Smokers have markedly higher rates of infection and delayed union.8 Cessation is strongly recommended several weeks prior to surgery. Likewise, surgeons should work to optimize conditions such as malnutrition, immunosuppression, and chronic steroid use whenever possible.
Adjacent Joint Deformity. Subtalar or midfoot malalignment such as cavovarus or planovalgus deformity can alter the mechanics of a TAR and lead to uneven loading.9 These deformities may require correction before or at the time of TAR. It is important to note that with hindfoot fusions, there is increased stress placed across the ankle implant, therefore recommendations exist to use a stemmed implant in this scenario.10
History of Prior Infection. As mentioned about in the absolute contraindications, patients with a prior ankle joint or adjacent infection are at greater risk for reactivation of that infection or chronic osteomyelitis. We have observed that a symptom-free interval of at least several years, with negative inflammatory markers, imaging, and even biopsies, is typically recommended before considering replacement. It may be possible to remove all chronically infected bone with the bone cuts during the total ankle procedure, thus eradicating the bone infection.
Young Age or High Activity Level. Although younger patients (<50 years) have shown encouraging short-term results, the long-term revision rate remains higher in this population.11 The lifetime mechanical demand simply exceeds the proven lifespan of most implants.12 For high-activity individuals, arthrodesis often provides a more durable solution with option for takedown conversion to total ankle at a later date.
Obesity. High body mass index (BMI) increases the mechanical load across the prosthesis, raising the risk of early failure. While not an absolute contraindication, surgeons should counsel patients with BMI >35 extensively about these risks and encourage them to pursue weight reduction prior to surgery.13
Ligamentous Laxity or Subluxation. One can correct moderate ligament instability during TAR with soft tissue balancing or reconstruction. However, if instability is severe or chronic, it may not be possible to maintain component alignment, making it a relative contraindication as long as instability is addressed intraoperativity.
Practical Evaluation Pointers for the Total Ankle Replacement Surgeon
Comprehensive History and Physical. A detailed history should include prior ankle injuries, surgeries, infections, wound problems, and medical comorbidities. Examine for deformity, range of motion, and ligamentous stability. Evaluate neurovascular status carefully palpate pulses, assess capillary refill, and test sensation.
Imaging and Diagnostics. Obtain weight-bearing radiographs of the ankle and hindfoot to assess alignment. Advanced imaging (CT or MRI) is valuable for evaluating bone loss or talar necrosis. When infection or vascular compromise is suspected, order appropriate labs or vascular studies (ABI/TBI).
Decision-Making. When multiple absolute contraindications are present, such as active infection, severe PVD, or neuropathy, one should avoid performing TAR. If only relative contraindications exist, surgeons should employ risk mitigation strategies before proceeding. Examples include smoking cessation, glycemic optimization, deformity correction, or staged surgery.
Preoperative Optimization. As part of the aforementioned decision-making, patients who ultimately undergo TAR should be medically optimized. This includes achieving good glycemic control (HbA1c <7.5%), cessation of nicotine products, treatment of nutritional deficiencies, and management of bone health. Weight reduction and physical conditioning may also improve postoperative recovery.
Pearls for Clinical Decision-Making
The following pearls are among those we have found valuable in our practice when looking at the impact of challenges or contraindications to total ankle replacement.
- Address alignment before replacement. Varus or valgus deformity exceeding 15° should be corrected via osteotomy or fusion before implanting a TAR.
- Prioritize soft tissue health. A pristine wound environment is non-negotiable; small ulcers or fragile skin should be fully healed before surgery.
- Be realistic with patients. Emphasize that TAR restores motion but not necessarily athletic performance, and implant longevity is finite.
- Consider long-term implications. In younger or high-activity patients, plan for the eventual need for revision or conversion to arthrodesis.
- Collaborate across disciplines. Coordination between podiatry, vascular surgery, endocrinology, and rehabilitation improves outcomes in high-risk patients.
Evolving Perspectives
We have seen many historical contraindications soften over time. Improved implant design and surgeon experience have made TAR possible in patients once deemed unsuitable. Younger age, mild deformity, and even moderate bone loss are no longer automatic exclusions when managed appropriately. Surgeons should always keep in mind, however, that the procedure demands precision, careful patient selection, and lifelong surveillance.
Dr. Ng specializes primarily in Foot and Ankle Reconstructive Surgery and Trauma. He is a Past President of ACFAS and ABFAS and current President of The Greater Texas Education Foundation.
Dr. Knauer is currently completing the Rocky Mountain Reconstructive Foot and Ankle Fellowship, where he focuses on complex deformity correction, arthrodesis, total ankle replacement, and advanced limb reconstruction.
Disclosures
Dr. Ng discloses that is he a consultant for Restor3d and Paragon 28/Zimmer Biomet. Dr. Knauer has no relevant disclosures.
References
1. Wang S, Qian Z, Liu X, et al. Effects of additional weight-bearing on the in vivo kinematics of the human ankle joint complex during walking. Sci Rep. 2024 Nov 23;14(1):29049. doi: 10.1038/s41598-024-80716-4. PMID: 39580514; PMCID: PMC11585603.
2. Suh DH, Han K, Lee JW, et al. Risk factors associated with failure of total ankle arthroplasty: a nationwide cohort study. Sci Rep. 2021 Feb 3;11(1):2878. doi: 10.1038/s41598-021-82674-7. PMID: 33536553; PMCID: PMC7859193.
3. Müller AM, Toepfer A, Harrasser N, et al. Significant prevalence of peripheral artery disease in patients with disturbed wound healing following elective foot and ankle surgery: Results from the ABI-PRIORY (ABI as a PRedictor of Impaired wound healing after ORthopedic surgerY) trial. Vasc Med. 2020 Apr;25(2):118-123. doi: 10.1177/1358863X19883945. Epub 2019 Nov 15. PMID: 32366205.
4. Vauclin CP, Berken D. Ankle Arthroplasty. [Updated 2024 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK606105/
5. Valan B, Anastasio AT, Kim Bet al. The INVISION Talar component in revision total ankle arthroplasty: analysis of early outcomes. Diagnostics (Basel). 2024 Jul 26;14(15):1612. doi: 10.3390/diagnostics14151612. PMID: 39125488; PMCID: PMC11311589.
6. Halai MM, Pinsker E, Mann MA, Daniels TR. Should 15° of valgus coronal-plane deformity be the upper limit for a total ankle arthroplasty? Bone Joint J. 2020 Dec;102-B(12):1689-1696. doi: 10.1302/0301-620X.102B12.BJJ-2020-0140.R1. PMID: 33249899.
7. Palanca A, Mann RA, Mann JA, Haskell A. Scandinavian Total Ankle Replacement: 15-year follow-up. Foot Ankle Int. 2018 Feb;39(2):135-142. doi: 10.1177/1071100717738747. PMID: 29389250.
8. Beahrs TR, Reagan J, Bettin CC, Grear BJ, Murphy GA, Richardson DR. Smoking effects in foot and ankle surgery: an evidence-based review. Foot Ankle Int. 2019 Oct;40(10):1226-1232. doi: 10.1177/1071100719867942. Epub 2019 Aug 18. PMID: 31423824.
9. Piga C, Maccario C, D'Ambrosi R, Romano F, Usuelli FG. Total ankle arthroplasty with valgus deformity. Foot Ankle Int. 2021 Jul;42(7):867-876. doi: 10.1177/1071100720985281. Epub 2021 Feb 1. PMID: 33517787.
10. Prissel MA, Hyer CF, Berlet GC. A review of 399 total ankle replacements: analysis of ipsilateral subtalar joint arthrodesis and associated talar component subsidence. J Foot Ankle Surg. 2017 Jan-Feb;56(1):10-14. doi: 10.1053/j.jfas.2016.10.004. PMID: 27989336.
11. Demetracopoulos CA, Adams SB Jr, Queen RM, DeOrio JK, Nunley JA 2nd, Easley ME. Effect of age on outcomes in total ankle arthroplasty. Foot Ankle Int. 2015;36(8):871-880. doi:10.1177/1071100715579717
12. Brunner S, Barg A, Knupp M, et al. The Scandinavian total ankle replacement: long-term, eleven to fifteen-year, survivorship analysis of the prosthesis in seventy-two consecutive patients. J Bone Joint Surg Am. 2013;95(8):711-718. doi:10.2106/JBJS.K.01580
13. Barg A, Knupp M, Anderson AE, Hintermann B. Total ankle replacement in obese patients: component stability, weight change, and functional outcome in 118 consecutive patients. Foot Ankle Int. 2011 Oct;32(10):925-32. doi: 10.3113/FAI.2011.0925. PMID: 22224320.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.





