


Superficial Venous Arterialization as an Alternative to Deep Venous Arterialization for Complex Limb Salvage
For patients with chronic limb-threatening ischemia (CLTI) who lack conventional revascularization options, venous arterialization offers a potential path to limb salvage. While deep venous arterialization (DVA) has gained attention in recent years, this case highlights superficial venous arterialization (SVA) as a viable alternative in a high-risk patient with diabetes and Rutherford 5 arterial disease. The report underscores procedural considerations, wound management strategy, and clinical outcomes supporting SVA as an emerging option for “no-option” limb preservation.
Key Takeaways
- Superficial venous arterialization (SVA) may offer a viable limb salvage option for “no-option” CLTI patients. In patients with severe tibial occlusive disease and no bypass targets, SVA can provide perfusion sufficient to support wound healing and functional recovery when traditional endovascular or surgical revascularization is not feasible.
- Successful outcomes depend on meticulous postoperative wound management and circuit maturation. Venous arterialization circuits require 4–6 weeks to mature. Aggressive wound care, staged surgical decision-making, and avoidance of premature flap closure are critical to optimizing perfusion and preventing reconstruction failure.
- While most literature focuses on DVA, SVA warrants further comparative investigation. Published limb salvage rates for venous arterialization range from 70% to 81%, yet data remains limited. This case supports the need for prospective studies comparing SVA and DVA techniques, standardized protocols, and long-term outcome tracking in complex limb preservation populations.
Chronic limb-threatening ischemia (CLTI), defined as ischemic rest pain or tissue loss, is a severe manifestation of peripheral artery disease.1 Often, CLTI presents as persistent pain at rest and wounds that fail to heal, sometimes accompanied by tissue death (classified as Rutherford categories 4-6). Due to their significant peripheral artery disease or anatomy, approximately 1 in 5 patients with CLTI cannot undergo standard blood vessel restoration procedures through minimally invasive or traditional surgical methods. These limitations stem from the positioning of arterial blockages, absence of suitable bypass targets or graft materials, or serious underlying health conditions, often leaving leg amputation as the sole remaining surgical intervention.2 Given amputation's substantial physical and emotional consequences, along with mortality rates ranging from 52% to 80% within 5 years, preserving the limb remains the primary treatment objective.3 With 50 to 100 new CLTI cases occurring per 100,000 American adults annually and mortality rates reaching 20%, identifying effective surgical solutions presents considerable challenges.4
Among these complex cases, patients with diabetes mellitus (DM) face particularly challenging circumstances, as DM significantly worsens the prognosis for patients with CLTI, increasing the risk by 2-4 times compared to patients with peripheral arterial disease (PAD) but without diabetes.5 Healing diabetic foot ulcerations (DFU) requires adequate arterial blood flow directly to the affected tissue. Patients with diabetes often develop severe blockages in the small distal arteries, leaving them without conventional revascularization treatment options.6 For these "no-option" patients with CLTI and diabetic foot ulcers, venous arterialization (VA) has emerged as a promising alternative approach for preventing limb amputation.
While catheter-based surgical interventions have advanced significantly, the prevalence of accompanying conditions like diabetes, high blood pressure, and kidney dysfunction has simultaneously risen, complicating traditional revascularization approaches and frequently rendering them unsuitable. This situation often results in persistent pain and nonhealing wounds due to inadequate blood flow, leading to amputation referrals.7
In response to this critical need for alternative approaches in seemingly nonsalvageable cases, vein arterialization (VA) has emerged as an innovative revascularization strategy that creates a connection between an upstream arterial blood source and a downstream venous drainage point to supply blood to the lower extremity, potentially providing treatment for patients who would otherwise face amputation.8,9 This report describes a patient with Rutherford category 5 CLTI who lacked viable endovascular or conventional surgical revascularization options and successfully received superficial vein arterialization (SVA) treatment for limb preservation.

Details of the Clinical Case
We present a case of a 72-year-old female with past medical history of coronary artery disease, type 2 diabetes mellitus, atrial fibrillation, hyperlipidemia, and extensive peripheral artery disease, previously deemed “no option” for vascular reconstruction. She developed and had undergone treatment for multiple wounds on her right foot and numerous infections. A diagnostic angiogram identified no surgical revascularization target in the foot, which resulted in a referral for a venous arterialization procedure. With worsening wounds and no traditional option for limb salvage, she underwent a superficial venous arterialization (SVA) as a last option for potential limb salvage.
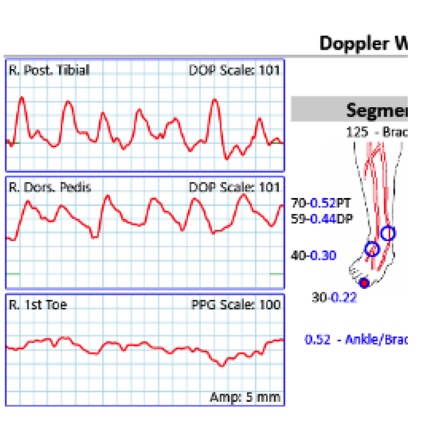
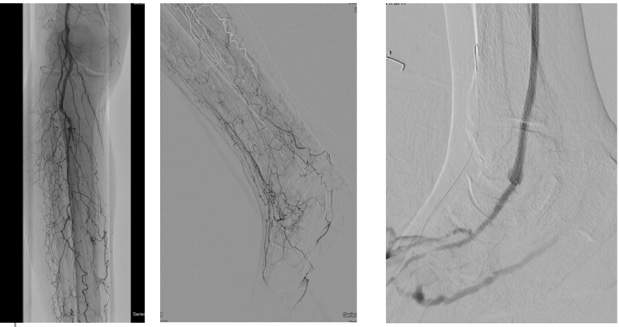
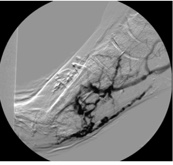
As in many cases, the patient presented with a relatively small (0.5cm x 0.5cm x 0.2cm) DFU under the first metatarsal on the right foot (Figure 1a, b). Over 2 months, the DFU did not close, instead, it grew with increasing depth to 0.4cm and developed osseous involvement. On her second hospitalization there was concern of DFU infection, and she underwent vascular imaging to assess the extent of her peripheral arterial disease (PAD). Her ankle brachial indices (ABIs) were falsely elevated due to her comorbidities and toe pressure was less than 40mmHg (Figure 2). Duplex ultrasound showed significant mural calcification of the tibial arteries of the right calf with occlusion of the right posterior tibial artery in the proximal calf and the right anterior tibial and peroneal arteries in the distal calf. Angiogram demonstrated severe tibial disease not amenable to endovascular interventions with no bypass target available (Figure 3). As described in the article by Montero-Baker and colleagues,10 given her occluded anterior tibial artery and suitable great saphenous vein, she underwent a hybrid superficial venous arterialization for limb salvage (Figure 4).
Post-surgical intervention, she continued aggressive local wound care while the SVA matured with biweekly follow-ups with vascular or podiatry. The VA circuit typically takes 4-6 weeks for maturation, during which time the new circuit powers the collateral circulation and tissues to achieve adequate oxygen delivery from the new arterialized vein.8 Prior to partial foot amputation, the patient had a repeat angiogram to detect any changes in blood flow that could jeopardize the patency of this reconstruction and, consequently, impair wound healing. The test revealed adequate perfusion.
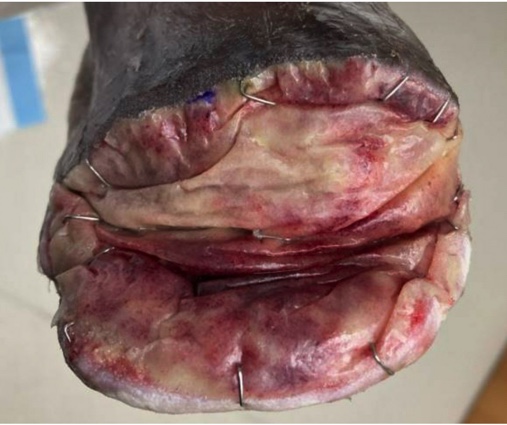
We eventually converted the original plan of a right foot sesamoidectomy to a transmetatarsal amputation (TMA) due to wound dehiscence and lack of progression. During the TMA, bone margins were cultured and biopsied with bacterial colonization evident and rather than reapproximating the flaps, we chose to augment healing by secondary intention. To achieve this, we used a biodegradable temporizing matrix (NovoSorb BTM, PolyNovo) followed by negative pressure wound therapy (NPWT) at -75mmHg initially for 1 week followed by -125mmHg thereafter with serial dressing changes performed twice weekly by home nursing and overlapping with clinic visits. Over the next 6 weeks, the wound developed healthy granulation tissue and became more superficial. The patient achieved complete healing with standard of care including weekly debridement five months post-revascularization (Figure 5).

Discussion
Peripheral artery disease (PAD) affects over 10 million Americans and 200 million worldwide, with 5% to 10% of these individuals developing chronic limb-threatening ischemia (CLTI), necessitating advanced interventional procedures like vein arterializations (VA) for limb preservation. VAs offer a treatment alternative for patients with "no-option" CLTI who have exhausted conventional therapeutic approaches.11
Historical development and technical approaches have undergone significant evolution since the technique's inception. The deep venous arterialization (DVA) technique, which involves creating a conduit to the venous system to enhance arterial circulation in the extremities, was initially described in 1912.9 While both open surgical and endovascular approaches have been employed over the decades, VAs have emerged as an endovascular solution at select centers, particularly as patient comorbidities have become more complex and increasing numbers of patients with CLTI lack viable surgical alternatives. Although our case utilized superficial vein arterialization (SVA), the majority of published literature focuses on deep venous arterialization (DVA) procedures, which have demonstrated promising outcomes in clinical studies.
Clinical evidence supporting VA techniques continues to accumulate, although the data remains limited.
In a study by Kum and colleagues, 7 high-amputation-risk patients with CLTI who had no conventional endovascular or surgical revascularization options underwent DVA.13 All patients achieved successful outcomes without amputations, experiencing resolution of claudication symptoms and improvements in wound healing following the procedure. Montero-Baker and colleagues noted that VA provides a previously unavailable treatment option for patients with no-option CLTI.. Limb salvage rates have been cited between 70% and 81%, with complete wound healing rates of 46% to 68% in 12 months.12,13

Despite these encouraging results, the need for larger-scale validation remains critical. Given VA's limited use, additional research is essential to evaluate this intervention and monitor long-term results. The ongoing PROMISE II trial is evaluating VA effectiveness using the LimFlow system in patients with CLTI that do not have other endovascular or open surgical alternatives.2 This study will track complication rates and long-term outcomes, providing crucial data on VA results. Potential VA complications include conduit thrombosis, loss of patency, and limb loss. This case study further highlights the meticulous wound care required after these revascularizations and underscores the need to resist the urge for early closure of skin flaps in this setting.

Concluding Notes
This case demonstrates that superficial vein arterialization (SVA) can achieve successful limb salvage in patients with no-option CLTI and diabetic foot ulcers who have exhausted conventional revascularization options. While most published literature focuses on deep venous arterialization (DVA), our patient's successful outcome with SVA including wound healing, functional ambulation, and pain resolution suggests this technique warrants further investigation as an alternative approach. Future research should include prospective studies with standardized protocols, more extended follow-up periods, objective perfusion measurements, and comparative studies between DVA and SVA approaches.
Dr. Nagarstheth is a Professor in the Department of Surgery, Division of Vascular Surgery, at the University of Maryland School of Medicine, where he is also the Medical Director of the Office-Based Laboratory. He is the Medical Director of C5E – Vascular Surgery Progressive Care Unit, the Co-Director of the UMSOM Limb Preservation program, the Associate Director of the Vascular Surgery Fellowship program, and Associate Director of the NIH Vascular Imaging Core Lab, all at the University of Maryland School of Medicine.
Dr. Dunlap is a Nurse Practitioner in the Department of Surgery, Division of Vascular Surgery, at the University of Maryland School of Medicine.
Dr. Fitzpatrick is a Nurse Practitioner in the Department of Surgery, Division of Vascular Surgery, at the University of Maryland School of Medicine.
Dr. Wynes is the Chief of Podiatric Services in the Department of Orthopaedics, Division of Podiatry, at the University of Maryland School of Medicine. He is the Co-Director of the UMSOM Limb Preservation program, and Program Director of the Limb Preservation and Deformity Correction Fellowship.
References
1. Srinivasan A, Miranda J, Mills JL. Appropriate care in chronic limb threatening ischemia: a review of current evidence and outcomes. Semin Vasc Surg. 2024;37(2):249-257.
2. The PROMISE II trial: percutaneous deep vein arterialization for the treatment of late-stage chronic limb-threatening ischemia. ClinicalTrials.gov identifier: NCT03970538.
3. Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45(suppl S):S5-S67.
4. Katib N, Thomas SD, Lennox AF, Yang JL, Varcoe RL. An endovascular-first approach to the treatment of critical limb ischemia results in superior limb salvage rates. J Endovasc Ther. 2015;22(4):473-481.
5. Shatnawi NJ, Al-Zoubi NA, Al-Bakkar LA, et al. Chronic limb-threatening ischemia in patients with type 2 diabetes: revascularization index as a predictor for primary endovascular intervention outcome. Vasc Health Risk Manag. 2023;19:495-504.
6. Spiliopoulos S, Davoutis E, Arkoudis NA, Sritharan K, Lechareas S. Percutaneous deep venous arterialization for limb salvage in no-option patients with chronic limb-threatening ischemia. J Clin Med. 2023;12(23):7324. doi:10.3390/jcm12237324
7. Ho VT, Gologorsky R, Kibrik P, et al. Open, percutaneous, and hybrid deep venous arterialization technique for no-option foot salvage. J Vasc Surg. 2020;71(6):2152-2160.
8. Clair D, Shishehbor MH, Trabal JM, Schreve M, Montero-Baker M, Lepow B, Ferraresi R. LimFlow percutaneous deep vein arterialization. Endovasc Today. 2021.
9. Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines. Circulation. 2006;113(11):e463-e654.
10. Montero-Baker M, Sommerset J, Miranda JA. Hybrid superficial venous arterialization and endovascular deep venous arterialization. J Vasc Surg Cases Innov Tech. 2023;9(3):101160. doi:10.1016/j.jvscit.2023.101160
11. Randial-Pérez LJ, Portilla-Rojas E, Pinzón-Pinto M, et al. Open distal venous arterialization technique as an opportunity for patients with critical limb ischemia: a Latin American experience. Vasc Endovascular Surg. 2025;59(4):428-434.
12. Montero-Baker M, Sommerset J, Miranda JA. Hybrid superficial venous arterialization and endovascular deep venous arterialization. J Vasc Surg Cases Innov Tech. 2023;9(3):101160.
13. Kum S, Tan YK, Schreve MA, et al. Midterm outcomes from a pilot study of percutaneous deep vein arterialization for the treatment of no-option critical limb ischemia. J Endovasc Ther. 2017;24(5):619-626.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.





