Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Kayla Wong BSa; Jennifer Nguyen BS, CCRCa; Evan Walser-Kuntz MSa; Sara Olson RN, CCRCa; Le Nguyen BSa; Tremayne Ansani BSa; Andrew Willett BSa; Mario Gössl MD, PhD, MHAa,b
From aMinneapolis Heart Institute Foundation, Minneapolis, Minnesota; bMinneapolis Heart Institute at Abbott Northwestern Hospital, Minneapolis, Minnesota
Acknowledgements: The authors would like to thank the research and statistical staff at Minneapolis Heart Institute Foundation for their assistance in data collection and analysis.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Clinical Summary
• Design/Population: Per Cath Lab Digest (2025), a retrospective cohort of 277 TAVR recipients with moderate–severe mitral regurgitation (MR) (192 functional [FMR]; 85 degenerative [DMR]) was followed for up to 5 years post TAVR to compare MR progression and clinical outcomes.
• Key Outcomes: FMR showed greater MR improvement (median −2 grades) vs DMR (−1 grade; p=.019), while DMR had higher 5-year mitral valve intervention incidence (13% vs 4.7%; p=.047). Mortality trended higher in DMR (hazard ratio 1.37; p=.075).
• Clinical Relevance/Limitations: Findings suggest etiology-specific MR trajectories may guide surveillance and downstream mitral valve planning, though results are limited by single-center design, semi-quantitative MR grading, and lack of multivariable adjustment.
Introduction
Transcatheter aortic valve replacement (TAVR) is a minimally invasive procedure that is commonly performed on patients with severe, symptomatic aortic stenosis (AS). Although TAVR was first established as a treatment option for these patients at high risk for surgical options, it has been shown to be a safe and effective alternative for patients of all risk stratifications.1 Among patients undergoing TAVR, up to 33% of them also experience concomitant more-than-mild mitral regurgitation (MR).2 However, there are different etiologies of mitral regurgitation, including degenerative MR (DMR) and functional MR (FMR). Mixed forms of MR may be present when features of both etiologies coexist; in this study, such cases were assigned to the most likely category based on clinical interpretation. Current findings suggest that over one-half of TAVR recipients with MR will experience an improvement in MR after TAVR.3 TAVR has expanded the number of therapeutic possibilities available for patients with AS and MR who are not suitable candidates for surgical procedures.4 However, little is known about the differential effects of TAVR on DMR and FMR. The few studies that have investigated the distinction between the impacts of TAVR on DMR and FMR evaluate the clinical outcomes and MR progression for 2 years after TAVR.5,6 A thorough assessment, including patients’ baseline characteristics along with MR severity and mechanism is required to develop an optimal treatment plan.7 This study aimed to compare patient characteristics between patients with FMR versus DMR, and estimate and compare their rate of MR progression 5 years after TAVR.
Methods
STUDY POPULATION
A retrospective study of 683 patients who received TAVR at Allina Health Minneapolis Heart Institute between 2014 and 2022 was conducted to analyze the patient characteristics and clinical outcomes of patients with DMR and FMR. Out of 683 patients, 277 patients met inclusion criteria of moderate to severe MR, including 192 patients with FMR and 85 patients with DMR. MR severity and dysfunction were quantified using transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE). Analysis of the degree and etiology of MR was performed by an accredited, board-certified expert reader in echocardiography according to American Society for Echocardiography (ASE) criteria. Formalized quantitative criteria could not be retrospectively applied.
DATA COLLECTION
Data were collected from Allina Health’s Electronic Data Warehouse (EDW). This included patient demographic data, medical history, and medications at the time of the procedure. Echocardiography assessments were analyzed pre TAVR, immediately post TAVR, and at follow-ups extending up to 5 years post TAVR. Because loading conditions and hemodynamics fluctuate significantly immediately after TAVR, early MR assessments should be interpreted with caution. Follow-up echocardiographic evaluations primarily focused on changes in MR severity and left ventricular ejection fraction (LVEF). Patient charts were reviewed for cardiac-related hospitalizations, incidence of stroke, mitral valve (MV) interventions, and all-cause mortality risk.
STUDY ENDPOINTS
The primary endpoint of this study was the change in MR grade severity following TAVR. Secondary endpoints included all-cause mortality, incidence of stroke, congestive heart failure (CHF) admission, and the need for MV interventions following TAVR.
STATISTICAL ANALYSES
Continuous variables were expressed as median (IQR) and compared across MR groups using Wilcoxon’s rank sum test. Categorical variables were expressed as frequency (%) and compared using either the chi-squared test or Fisher’s exact test where appropriate. Cumulative incidence was used to estimate the incidence of MV interventions, which was compared across MR groups using Gray’s test. Changes in LVEF and MR grade before and after TAVR were compared using Wilcoxon’s rank sum test. The frequency of all-cause mortality was estimated using the Kaplan-Meier method, and the risk of death between the MR groups was compared using a Cox proportional hazards model. All analyses were conducted in R version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
BASELINE CHARACTERISTICS
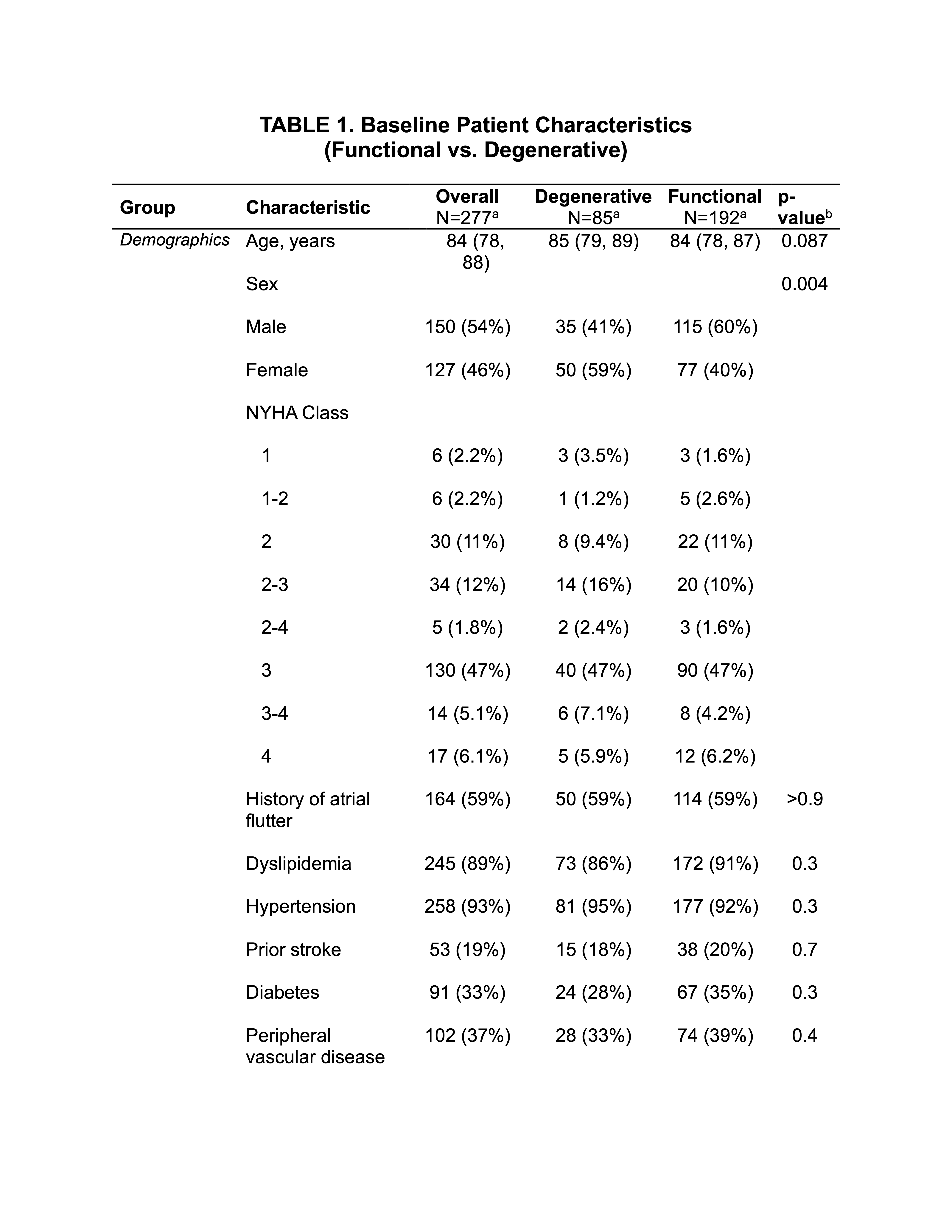
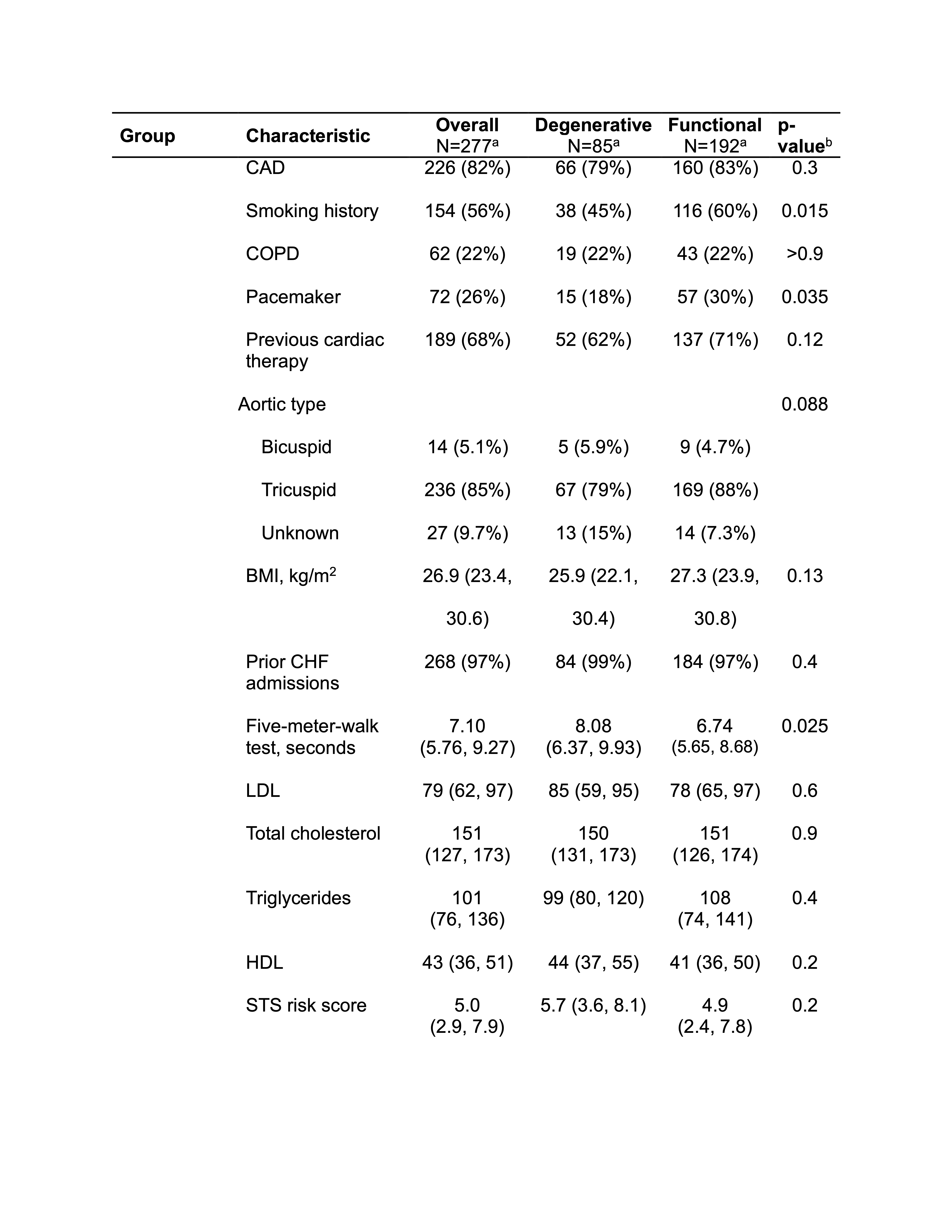
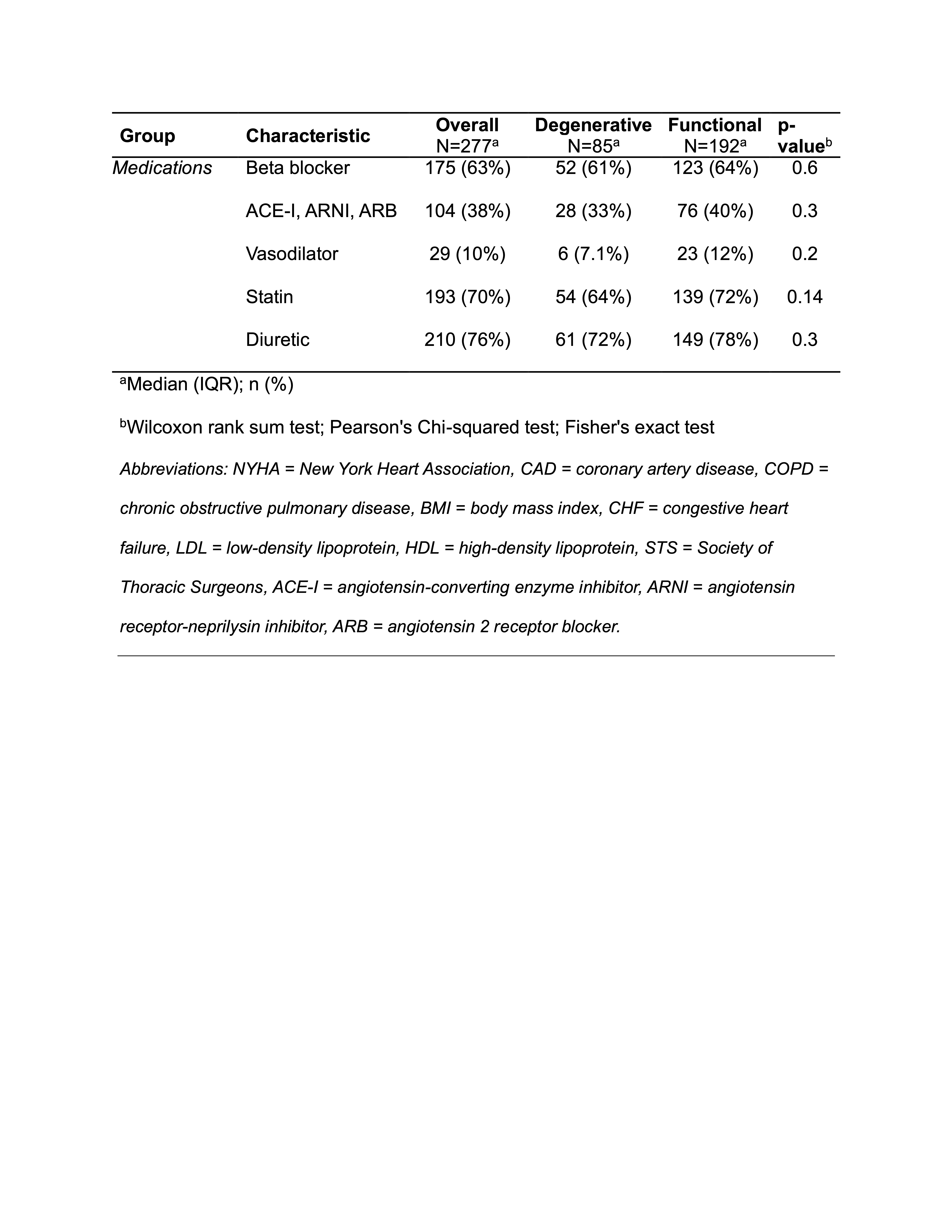
Out of 277 patients who met inclusion criteria, 192 patients were categorized as FMR, and 85 patients as DMR. The mean age across groups was 84 ± 4 years (Table 1). Among DMR patients, 35 (41%) were male, whereas 115 (60%) of FMR patients were male. Preoperatively, 72 (26%) patients had a history of pacemaker implantation, with 57 (30%) patients in the FMR group and 15 (18%) patients in the DMR group. Results from the 5-meter-walk-test show a significant difference in average completion time (6.74 seconds for FMR vs. 8.08 seconds for DMR, p=.025). Information on prior and current medications taken at the time of the procedure was also collected:
• 210 (76%) patients were taking diuretics,
• 193 (70%) patients were on a statin,
• 175 (63%) patients were on beta blocker,
• 104 (38%) patients were receiving an angiotensin-converting enzyme inhibitor (ACE-I), angiotensin receptor blocker (ARB), or angiotensin receptor-neprilysin inhibitor (ARNI), and
• 29 (10%) were on a vasodilator.
OUTCOMES AT 5 YEARS
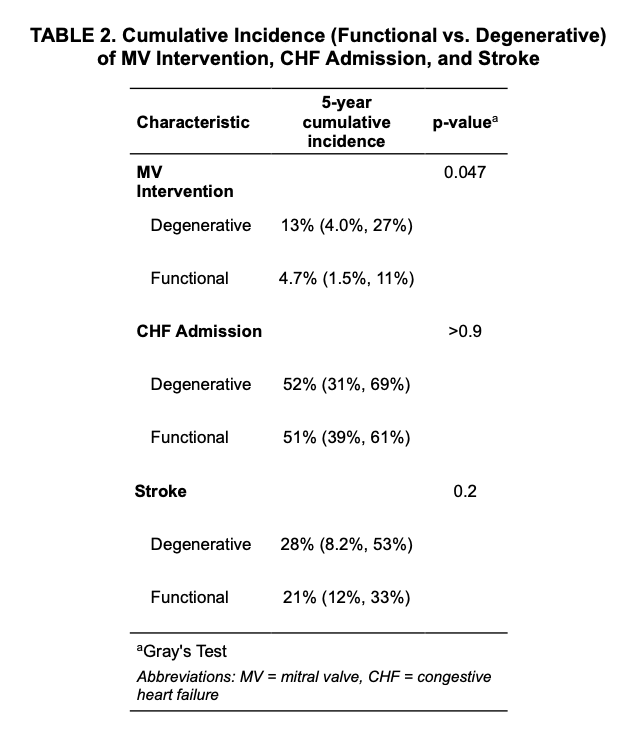
Cumulative incidence for MV intervention, congestive heart failure (CHF) admission, and stroke were compared between FMR and DMR groups. Within 5 years post TAVR, the cumulative incidence of MV intervention was significantly higher in DMR patients (13%) compared to FMR patients (4.7%, p=.047; Table 2). There was no significant difference in cumulative incidence of CHF admission within 5 years post TAVR, with 51% in FMR patients compared to 52% in DMR patients (p>.9). Additionally, there was no significant difference in stroke rates between the two groups (21% in FMR vs. 28% in DMR, p=.2).
VALVE DETERIORIATION OUTCOMES
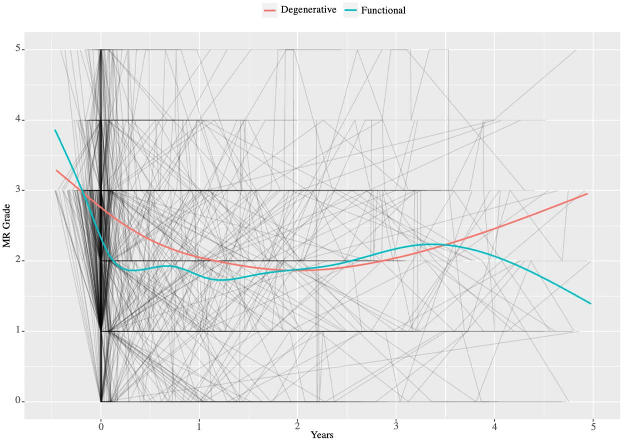
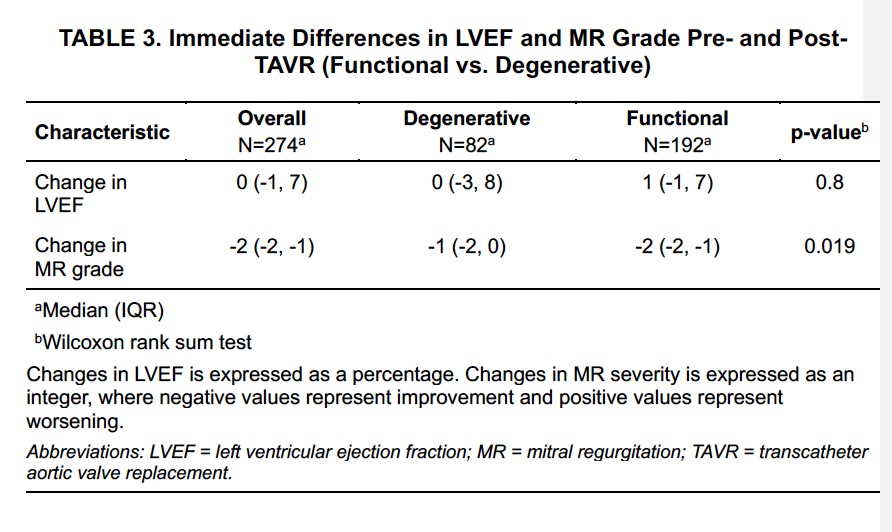
Quantitative differences between LVEF and MR grade severity pre and post TAVR were compared across FMR and DMR groups. While there was no significant difference in LVEF pre and post TAVR between groups, there was a significant finding in the difference between MR severity pre and post TAVR between the two groups. FMR patients demonstrated a median improvement of two MR grades, while DMR patients showed a median improvement of one grade on the semi-quantitative MR scale when comparing echocardiography pre- and post-TAVR (p=.019; Table 3). At ~3.5 years post-TAVR, FMR patients showed a continued trend toward improvement in MR severity, approaching the less-than-mild category (Figure 1). In contrast, DMR patients showed a trend toward progressive MR worsening, consistent with degenerative leaflet disease, with a gradual increase in MR grade severity over the subsequent 2 years.
Figure 1. MR Grade vs Time post TAVR.
Plot illustrating MR progression in all patients (gray lines), with a comparison of average MR progression among degenerative MR (red line) and functional MR (blue line) over 5 years post-TAVR. MR severity is measured as follows: 0 = none, 1 = mild, 2 = mild-moderate, 3 = moderate, 4 = moderate-severe, 5 = severe.
Results show that only functional MR patients experienced a sustained improvement after 5 years post-TAVR.
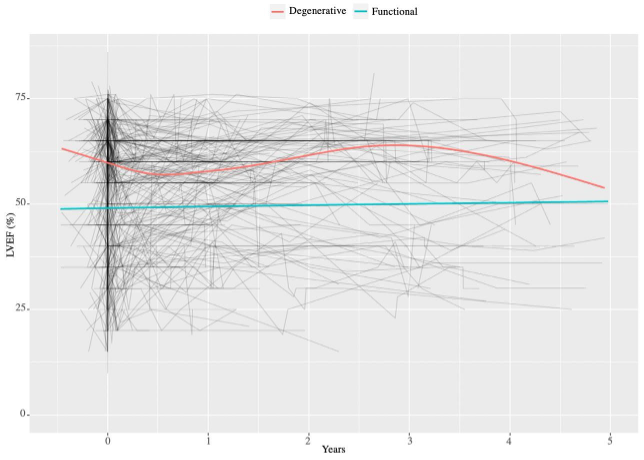
Throughout the 5-year follow up period, FMR patients demonstrated no significant change in LVEF (IQR: 1; 95% CI: -1 – 7, p=.8; Table 3). In contrast, DMR patients exhibited more pronounced fluctuations in LVEF, initially averaging 62%, then decreasing to 55%, though not falling below 50% over the 5-year span (Figure 2). There was a trend toward increased mortality in the DMR group compared to the FMR group (HR 1.37, 95% CI 0.97–1.94; p=.075), though this did not reach statistical significance.
Figure 2. LVEF vs Time Post TAVR.
Plot depicting changes in LVEF in all patients (gray lines), with a comparison of the average change in LVEF among degenerative MR (red line) and functional MR (blue line) over 5 years post-TAVR. LVEF is expressed as a percentage.
Results indicate that LVEF does not change significantly in functional MR patients over the 5-year follow-up period.
This retrospective single-center study characterizes MR progression in 277 patients who underwent TAVR over a five-year follow-up period. The results from this study highlight two key findings:
(1) FMR and DMR patients experienced a significantly different progression in MR post TAVR. Both groups experience a short-term improvement in MR about 1-year post-TAVR. However, long-term clinical trajectories differ between the two groups, driven primarily by more durable MR improvement in FMR and higher MV intervention rates in DMR. FMR patients experienced sustained improvement up to 5 years post-TAVR while DMR patients demonstrated progressive MR recurrence consistent with degenerative leaflet disease, placing them at higher likelihood of requiring MV intervention over long-term follow-up;
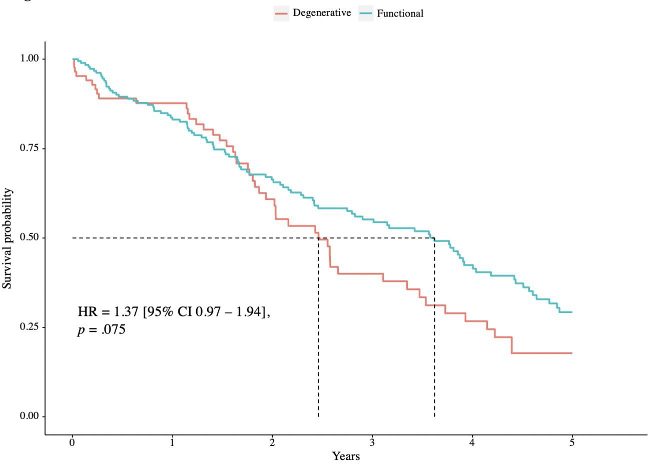
(2) DMR patients demonstrated a nonsignificant trend toward lower survival than FMR patients within 5 years post TAVR (Figure 3). These findings suggest that patients with severe AS and DMR may warrant closer longitudinal surveillance and may be more likely to require subsequent mitral intervention.
Figure 3. Survival Free of Death.
Comparison of Kaplan-Meier curves of survival from all-cause mortality following TAVR between degenerative MR (red line) and functional MR (blue line). Patients with degenerative MR demonstrated a non-significant trend toward higher mortality (HR 1.37, p = .075).
Abbreviations: HR = hazard ratio; CI = confidence interval.
The results of this study are consistent with existing literature, which indicates that patients undergoing TAVR who also have concomitant MR are at an increased risk of requiring an MV intervention within 5 years post TAVR.8 Our research extends the current evidence that DMR predicts worse outcomes in patients undergoing TAVR than FMR etiologies.5 Future studies should evaluate whether staged or combined mitral interventions after TAVR offer incremental benefit for DMR, such as mitral valve transcatheter edge-to-edge repair (M-TEER) and transcatheter mitral valve replacement (TMVR). TEER is a safe and well-established percutaneous intervention that treats primary and secondary MR.9-11 Recent literature has shown that TEER for MR has better outcomes when compared to conservative management.12 A large-scale nationwide analysis found that the number of patients who underwent M-TEER after recent TAVR each year in the United States is increasing along with the number of M-TEER procedures, due to its reduction of 30- and 90-day rates of acute care hospitalizations (ACH) and heart failure hospitalizations (HFH).13 In patients with high surgical risk, M-TEER may be a feasible and effective intervention to safely reduce MR and optimize clinical outcomes.14 A two-year observational study aimed to investigate the clinical outcomes of staged TEER for residual significant MR after TAVR found low in-hospital complication rates among patients who underwent TEER compared to those who did not, and a more substantial clinical benefit of a staged TEER after TAVR for those with DMR than FMR.15
Furthermore, when evaluating the feasibility of TEER after TAVR, research indicates no significant difference in in-hospital mortality between patients undergoing staged vs. concomitant TEER; however, complication rates are significantly higher in those undergoing concomitant TEER.16 Given these implications, it is vital to evaluate the clinical history of these patients when assessing for the possibility of TEER after TAVR.
Additionally, studies have demonstrated that TMVR is a potential safe alternative therapy for patients with symptomatic MR. One prospective study evaluating the safety and efficacy of TMVR with a self-expanding prosthesis in a cohort of high-surgical-risk patients found that the procedure safely reduced symptomatic MR within 30 days post TMVR.17 Similarly, a registry-based cohort study reported a procedural success rate of 88.9% in patients with isolated degenerative MR, further supporting the safety and effectiveness of TMVR.18
Collectively, emerging, investigative clinical evidence suggests that TMVR may address the limitations of other interventions, providing a viable treatment option for complex mitral valve diseases across a wide range of anatomical variations.19-21 This pattern of MR progression underscores the importance of further research into treatment strategies for patients with concomitant DMR undergoing TAVR. Future studies should evaluate whether multimodal approaches, including M-TEER or TMVR performed at or after TAVR, offer benefit in appropriately selected patients.
Study Limitations
This study has several limitations. First, it is a single-center, retrospective analysis with a sample size of 683 patients, of whom only 277 met the inclusion criteria. This may limit the generalizability of the findings. MR grading was based on routine clinical TTE/TEE reports using semi-quantitative criteria; lack of core-lab adjudication may introduce variability in MR classification and magnitude of change. Second, MR assessment can vary among physicians, and the reliance on retrospective interpretation of clinical notes introduces potential subjectivity, which may impact diagnostic accuracy. Additionally, assignment of MR etiology (DMR vs. FMR) relied on clinical interpretation rather than strict quantitative definitions, which may result in misclassification, particularly in patients with mixed features. Third, this study primarily differentiates between functional and degenerative MR and does not fully account for patients with mixed etiologies, which could influence these outcomes. Finally, cumulative incidence results are influenced by individual patient survival, ranging from 1 to 5 years post TAVR, leading to variable clinical trajectories that complicate direct comparisons. These factors must be considered when interpreting the study’s findings. Immediate post TAVR MR assessment may be influenced by procedural hemodynamics and should be interpreted cautiously. No multivariable adjustment was performed; therefore observed differences may be partially attributable to baseline clinical differences rather than MR etiology alone.
Conclusion
Patients with severe AS and concomitant moderate to severe MR may experience an improvement in MR after TAVR; however, this study demonstrates that the degree and durability of this improvement, along with other clinical outcomes, are dependent on MR etiology. Patients with DMR demonstrated higher rates of MV intervention and a non-significant trend toward increased mortality compared with those with FMR. Given these findings, further evaluation of optimal treatment strategies for patients with DMR undergoing TAVR is warranted. Future research should evaluate whether staged or combined MV interventions after TAVR may offer benefit in selected patients. Further investigation is needed to clarify the role and long-term implications of combined or staged interventions in this population.
References
1. Chiarito M, Spirito A, Nicolas J, et al. Evolving devices and material in transcatheter aortic valve replacement: what to use and for whom. J Clin Med. 2022 Jul 30;11(15):4445. doi:10.3390/jcm11154445
2. Nappi F, Nenna A, Timofeeva I, et al. Mitral regurgitation after transcatheter aortic valve replacement. J Thorac Dis. 2020 May;12(5):2926-2935. doi:10.21037/jtd.2020.01.69
3. Cortés C, Amat-Santos IJ, Nombela-Franco L, et al. Mitral regurgitation after transcatheter aortic valve replacement: prognosis, imaging predictors, and potential management. JACC Cardiovasc Interv. 2016 Aug 8;9(15):1603-14. doi:10.1016/j.jcin.2016.05.025
4. Davidson LJ, Davidson CJ. Transcatheter treatment of valvular heart disease: a review. JAMA. 2021 Jun 22;325(24):2480-2494. doi:10.1001/jama.2021.2133
5. Kindya B, Ouzan E, Lerakis S, et al. Degenerative mitral regurgitation predicts worse outcomes in patients undergoing transcatheter aortic valve replacement. Catheter Cardiovasc Interv. 2018 Sep 1;92(3):574-582. doi:10.1002/ccd.27607
6. Vollenbroich R, Stortecky S, Praz F, et al. The impact of functional vs degenerative mitral regurgitation on clinical outcomes among patients undergoing transcatheter aortic valve implantation. Am Heart J. 2017 Feb;184:71-80. doi:10.1016/j.ahj.2016.10.015
7. Tirado-Conte G, McInerney A, Jimenez-Quevedo P, et al. Managing the patient undergoing transcatheter aortic valve replacement with ongoing mitral regurgitation. Expert Rev Cardiovasc Ther. 2021 Aug;19(8):711-723. doi:10.1080/14779072.2021.1955347
8. Witberg G, Codner P, Landes U, et al. Effect of transcatheter aortic valve replacement on concomitant mitral regurgitation and its impact on mortality. JACC Cardiovasc Interv. 2021 Jun 14;14(11):1181-1192. doi:10.1016/j.jcin.2021.02.030
9. Layoun H, Harb SC, Krishnaswamy A, et al. Patient selection for mitral transcatheter edge-to-edge repair. Methodist Debakey Cardiovasc J. 2023 May 16;19(3):26-36. doi:10.14797/mdcvj.1199
10. Li Z, Yi F, Zuo K, et al. A review regarding the article 'clinical and echocardiographic outcomes of patients undergoing transcatheter edge-to-edge repair for functional vs degenerative mitral valve regurgitation'. Curr Probl Cardiol. 2024 Apr;49(4):102461. doi:10.1016/j.cpcardiol.2024.102461
11. Chiarito M, Pagnesi M, Martino EA, et al. Outcome after percutaneous edge-to-edge mitral repair for functional and degenerative mitral regurgitation: a systematic review and meta-analysis. Heart. 2018 Feb;104(4):306-312. doi:10.1136/heartjnl-2017-311412
12. Dokollari A, Sicouri S, Ridwan K, et al. Clinical and echocardiographic outcomes of patients undergoing transcatheter edge-to-edge repair for functional vs degenerative mitral valve regurgitation. Curr Probl Cardiol. 2024 Jan;49(1 Pt B):102064. doi:10.1016/j.cpcardiol.2023.102064
13. Elkaryoni A, Saad M, Darki A, et al. Mitral valve transcatheter edge-to-edge repair after TAVR: a nationwide analysis. Am J Cardiol. 2023 Dec 15;209:184-189. doi:10.1016/j.amjcard.2023.09.089
14. Hausleiter J, Stocker TJ, Adamo M, et al. Mitral valve transcatheter edge-to-edge repair. EuroIntervention. 2023 Jan 23;18(12):957-976. doi:10.4244/EIJ-D-22-00725.
15. Nagasaka T, Shechter A, Patel V, et al. Two-year clinical outcomes of staged transcatheter mitral edge-to-edge repair after transcatheter aortic valve replacement. Am J Cardiol. 2024 Aug 1;224:46-54. doi:10.1016/j.amjcard.2024.05.032
16. Zahid S, Khalouf A, Hashem A, et al. Safety and feasibility of staged versus concomitant transcatheter edge-to-edge mitral valve repair after transcatheter aortic valve implantation. Am J Cardiol. 2023 Apr 1;192:109-115. doi:10.1016/j.amjcard.2023.01.037
17. Muller DWM, Farivar RS, Jansz P, et al; Tendyne Global Feasibility Trial Investigators. Transcatheter mitral valve replacement for patients with symptomatic mitral regurgitation: a global feasibility trial. J Am Coll Cardiol. 2017 Jan 31;69(4):381-391. doi:10.1016/j.jacc.2016.10.068
18. Makkar RR, Chikwe J, Chakravarty T, et al. Transcatheter mitral valve repair for degenerative mitral regurgitation. JAMA. 2023 May 23;329(20):1778-1788. doi:10.1001/jama.2023.7089
19. Hensey M, Brown RA, Lal S, et al. Transcatheter mitral valve replacement: an update on current techniques, technologies, and future directions. JACC Cardiovasc Interv. 2021 Mar 8;14(5):489-500. doi:10.1016/j.jcin.2020.12.038
20. Ludwig S, Granada JF. Transcatheter mitral valve replacement at an inflection point: lessons learned and the path forward. Eur Heart J. 2024 May 27;45(20):1776-1778. doi:10.1093/eurheartj/ehae013.
21. Quentin V, Mesnier J, Delhomme C, et al. Transcatheter mitral valve replacement using transcatheter aortic valve or dedicated devices: current evidence and future prospects. J Clin Med. 2023 Oct 24;12(21):6712. doi:10.3390/jcm12216712
“This early feasibility study for J-Valve is encouraging," said Dean J. Kereiakes, MD, MSCAI. "It shows that a dedicated device designed for aortic regurgitation can achieve sustained valve performance, meaningful symptom improvement, and...
“This early feasibility study for J-Valve is encouraging," said Dean J. Kereiakes, MD, MSCAI. "It shows that a dedicated device designed for aortic regurgitation can achieve sustained valve performance, meaningful symptom improvement, and...
The most notable enhancement is the ability to view medical images directly within the app. This long-awaited feature enables care teams to review imaging in real time.
The most notable enhancement is the ability to view medical images directly within the app. This long-awaited feature enables care teams to review imaging in real time.
“Our new Institute will expand our efforts across the full spectrum of valvular heart disease,” Dr. Adams says. “Collaboration has been the foundation of our success, bringing together cardiologists, imaging specialists, anesthesiologists,...
“Our new Institute will expand our efforts across the full spectrum of valvular heart disease,” Dr. Adams says. “Collaboration has been the foundation of our success, bringing together cardiologists, imaging specialists, anesthesiologists,...
The study utilized Tempus Next, an AI platform that identifies significant AS or MR patients who may meet guideline-indicated therapy criteria, but do not have a treatment plan in place.
The study utilized Tempus Next, an AI platform that identifies significant AS or MR patients who may meet guideline-indicated therapy criteria, but do not have a treatment plan in place.
“This early feasibility study for J-Valve is encouraging," said Dean J. Kereiakes, MD, MSCAI. "It shows that a dedicated device designed for aortic regurgitation can achieve sustained valve performance, meaningful symptom improvement, and...
“This early feasibility study for J-Valve is encouraging," said Dean J. Kereiakes, MD, MSCAI. "It shows that a dedicated device designed for aortic regurgitation can achieve sustained valve performance, meaningful symptom improvement, and...
A pacemaker without a box under the skin. Without wires to the heart. And without a battery that needs to be replaced every 7-10 years. It sounds like something from the distant future, but Dutch researchers at biotech company PacingCure have...
A pacemaker without a box under the skin. Without wires to the heart. And without a battery that needs to be replaced every 7-10 years. It sounds like something from the distant future, but Dutch researchers at biotech company PacingCure have...
The U.S. IDE study program will evaluate the purpose-built Shockwave™ SkyRunner Carotid IVL System designed to address the challenges of calcification in carotid arteries prior to stenting.
The U.S. IDE study program will evaluate the purpose-built Shockwave™ SkyRunner Carotid IVL System designed to address the challenges of calcification in carotid arteries prior to stenting.
ARLINGTON, VA — The Society of Cardiovascular Computed Tomography (SCCT) selected Ido Avivi, MD as the second recipient of the Chinnaiyan Catalyst Award for Women's Cardiovascular Health Research.
The award — established in 2025 by SCCT...
ARLINGTON, VA — The Society of Cardiovascular Computed Tomography (SCCT) selected Ido Avivi, MD as the second recipient of the Chinnaiyan Catalyst Award for Women's Cardiovascular Health Research.
The award — established in 2025 by SCCT...
Junkosha, pioneers of sophisticated fluoropolymer application technologies, has concluded its highly successful third Technology Innovator of the Year Award through a live stream YouTube ceremony held on June 17th 2026. Up first was Dr....
Junkosha, pioneers of sophisticated fluoropolymer application technologies, has concluded its highly successful third Technology Innovator of the Year Award through a live stream YouTube ceremony held on June 17th 2026. Up first was Dr....
Key Highlights
The Volante Steerable Guiding Sheath is designed to facilitate intracardiac, renal and peripheral placement of diagnostic and therapeutic devices.
With five different lengths and six different French sizes,...
Key Highlights
The Volante Steerable Guiding Sheath is designed to facilitate intracardiac, renal and peripheral placement of diagnostic and therapeutic devices.
With five different lengths and six different French sizes,...
Treating patients within 12 hours of diagnosis may be associated with greater improvement in acute hemodynamic and right ventricle measures compared to treatment after 12 hours, with similar safety outcomes between groups.
Treating patients within 12 hours of diagnosis may be associated with greater improvement in acute hemodynamic and right ventricle measures compared to treatment after 12 hours, with similar safety outcomes between groups.
The most notable enhancement is the ability to view medical images directly within the app. This long-awaited feature enables care teams to review imaging in real time.
The most notable enhancement is the ability to view medical images directly within the app. This long-awaited feature enables care teams to review imaging in real time.
AK-AVS, which received FDA Breakthrough Device Designation in October 2024, is an ECG-based AI algorithm intended to aid in the diagnosis of moderate to severe aortic valve stenosis in adult patients 22 years and older, utilizing data derived...
AK-AVS, which received FDA Breakthrough Device Designation in October 2024, is an ECG-based AI algorithm intended to aid in the diagnosis of moderate to severe aortic valve stenosis in adult patients 22 years and older, utilizing data derived...