


Vascular Access and Mortality Outcomes: Insights From the Percutaneous Coronary Interventions Registry From the Netherlands Heart Registration
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
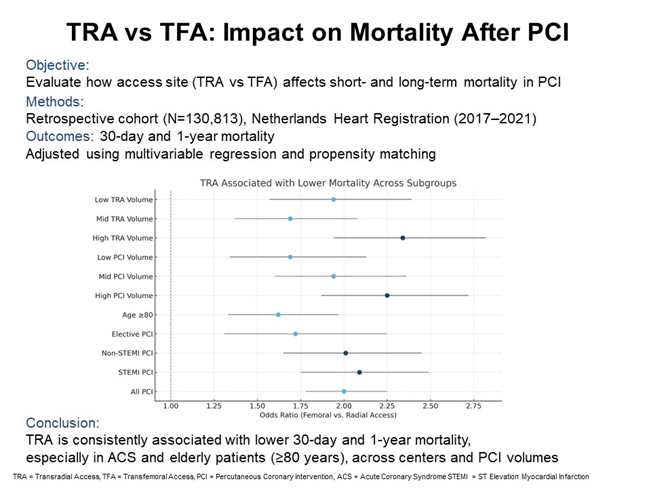
Objectives. While the transradial approach (TRA) is associated with fewer bleeding complications than the transfemoral approach (TFA), its effect on mortality outcomes in real-world clinical practice remains unclear. This study examines the relationship between vascular access site and mortality in patients undergoing percutaneous coronary intervention (PCI).
Methods. This retrospective cohort study used prospectively collected data from the Netherlands Heart Registration, including 130 813 PCI procedures between 2017 and 2021. The primary outcome was 30-day mortality and the secondary outcome was 1-year mortality. Outcomes were adjusted for baseline variables using multivariable logistic regression and matching propensity scores.
Results. TRA was more commonly used in younger male patients with acute coronary syndromes, while TFA was preferred in elective procedures and patients with prior coronary artery bypass grafting. TFA was associated with significantly higher mortality at 30 days (odds ratio [OR], 2.00; 95% CI, 1.78-2.25) and 1 year (OR, 1.50; 95% CI, 1.39-1.61). Mortality benefits with TRA were particularly pronounced in patients with acute coronary syndrome and those 80 years or older, and remained consistent across procedural volumes and center-level TRA adoption rates.
Conclusions. TRA is associated with lower short- and long-term mortality in PCI, supporting its broader adoption in routine clinical practice.
Introduction
The transradial approach (TRA) for coronary angiography and percutaneous coronary intervention (PCI) was first described in 1989 and 1993, respectively.1,2 Most interventional cardiologists now favor TRA over the traditional transfemoral approach (TFA) because of its association with lower rates of major bleeding complications.3,4 Evidence shows that TRA significantly reduces bleeding across elective and urgent procedures, in octogenarians, and in patients presenting with cardiogenic shock.5,6
While the link between TRA and reduced bleeding is well established, its association with mortality is less certain. Some studies suggest bleeding reduction may lead to lower mortality rates,3 though this has not been consistently validated in real-world settings.7 Trial data also indicate TRA benefits may depend on operator proficiency and center-specific TRA use.4 Additionally, the applicability of randomized trials to broader clinical practice is debated because of the strict inclusion criteria and use of highly experienced operators.4,7,8
Although international guidelines endorse TRA as a Class IA recommendation,9,10 the access decision remains operator-dependent. Therefore, observational real-world data are valuable to clarify the link between vascular access and clinical outcomes following PCI.
Methods
Study design
This retrospective multicenter cohort study used prospectively collected data from the Netherlands Heart Registration (NHR) PCI Registry. The study was approved by the institutional review board MEC-U (W19.270) and conducted in accordance with the Declaration of Helsinki; a waiver for informed consent was obtained.
The NHR is a national quality registry of invasive cardiac procedures from all Dutch hospitals. Data are extracted from electronic health records and recorded in a secure online environment in compliance with standardized definitions, available via www.nhr.nl. Prior publications describe the NHR’s data acquisition and quality control procedures.11-12
We investigated the relationship between vascular access and mortality in PCI, comparing TRA and TFA, while adjusting for case-mix. Subgroup analyses evaluated the effect of procedural volume and TRA experience at the center level.
Inclusion and exclusion criteria
We included all PCIs in patients 18 years or older that were performed in Dutch centers from January 1, 2017, to December 31, 2021. We excluded cases where the access site was undefined, alternative, or multiple access routes were used, and cases with procedures involving out-of-hospital cardiac arrest, cardiogenic shock, or chronic total occlusion (CTO).
Outcomes
The primary outcome was 30-day mortality; the secondary outcome was 1-year mortality. Mortality data came from the governmental Personal Records Database (Basisregistratie Personen). By limiting inclusion to procedures until the end of 2021, 1-year outcomes were complete and unaffected by the COVID-19 pandemic.
Statistical analyses
Baseline characteristics were compared between TRA and TFA. Continuous variables were presented as mean ± SD or median with IQR. Categorical variables were shown as counts with percentages. Statistical tests included t-tests, Mann-Whitney U-tests, chi-square tests, and Fisher’s exact tests. Trends over time and intercenter variation were also analyzed.
Binary logistic regression assessed the relationship between access route and mortality. Multivariable regression adjusted for key covariates. Missing data were imputed under the missing-at-random assumption using 20 iterations and 20 imputed datasets. Access route and 30-day mortality were included but not imputed.
Subgroup analyses were based on PCI indication (elective, non-ST-elevation myocardial infarction [NSTEMI], and STEMI), patient age (≥80 years), center procedural volume (high, medium, and low), and center TRA/TFA usage (tertiles). Odds ratios (ORs) with CIs and P-values were reported. Significance was defined as a P-value of less than 0.05.
A propensity score-matched (PSM) analysis was conducted as a sensitivity analysis. Propensity scores were estimated using all available baseline variables in 5 imputed datasets. Matching used the nearest neighbor method (caliper 0.01), with 1:1 matching of TRA to TFA cases. Mortality associations were then reassessed by logistic regression. The PSM analysis was performed using R Studio software, version 3.6.2 (R Foundation for Statistical Computing).
Results
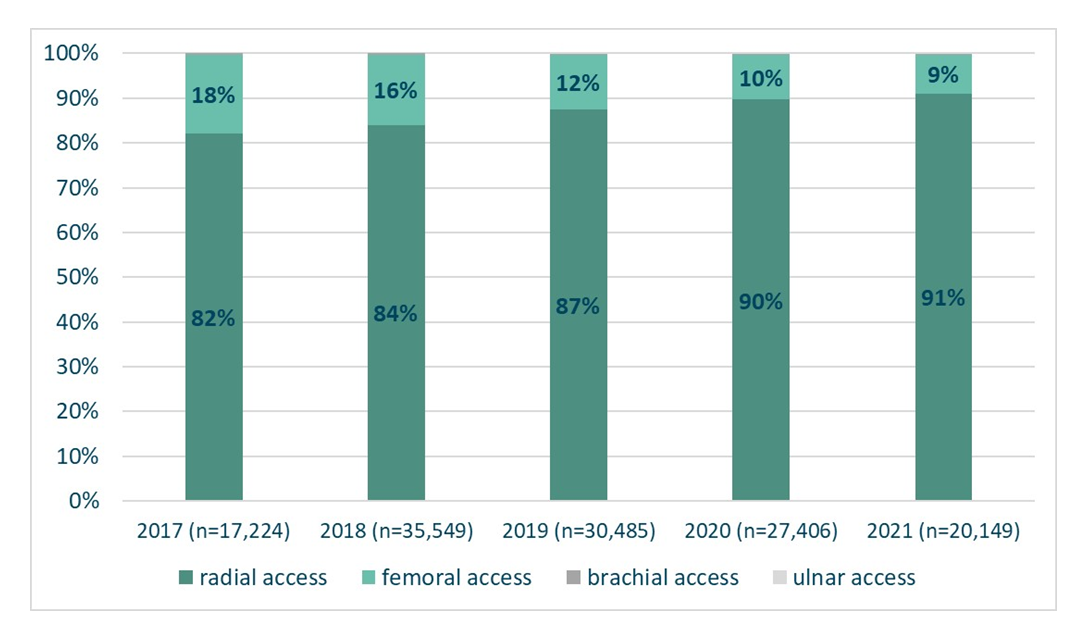
We included 130 813 patients (around 26 000 PCIs/year). TRA was dominant, increasing from 82% (14 124/17 224) of patients in 2017 to 91% (18 334/20 149) of patients in 2021 (Figure 1). The use of alternative accesses (brachial, ulnar) was negligible. The final study cohort consisted of 113 633 TRA and 16 786 TFA PCI patients.
Baseline characteristics
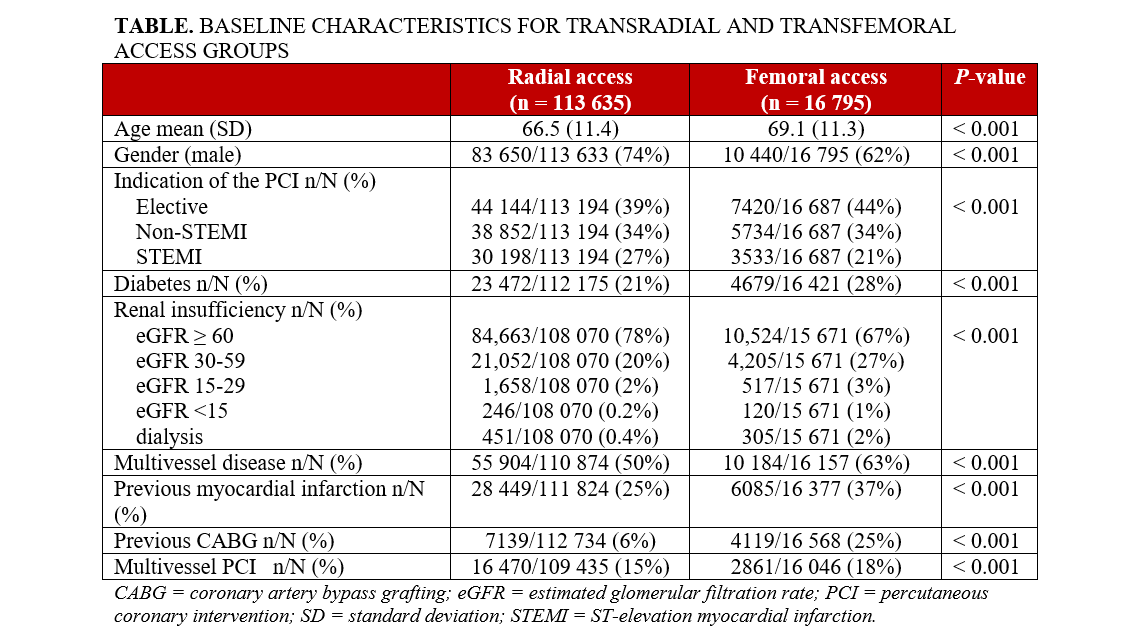
TRA patients were younger (66.5 vs 69.1 years), more often male (TRA: 83 650/113 633; 74% vs TFA: 10 440/16 795; 62%), and more likely to have acute coronary syndrome (ACS) and STEMI. TFA was more often used in elective procedures and patients with comorbidities including diabetes, impaired renal function, multivessel disease, previous MI, prior coronary artery bypass grafting (CABG), and multivessel PCI (Table).
Short and long-term mortality
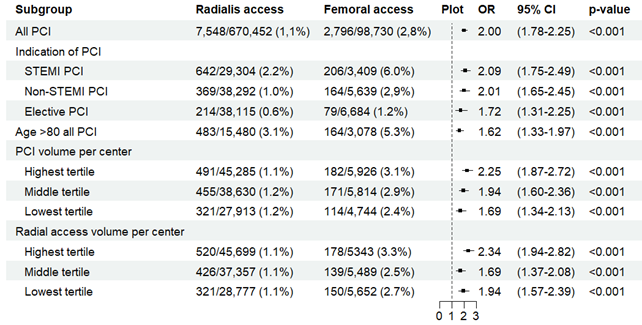
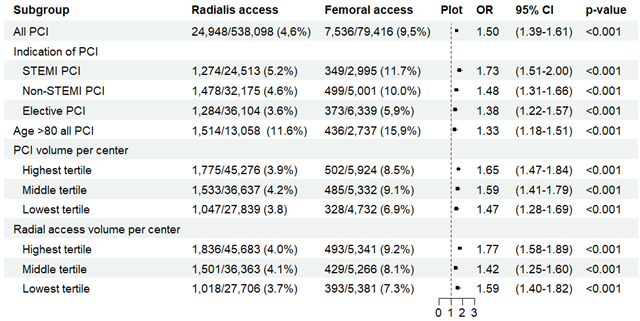
Thirty-day mortality was 1.1% (7548/670 452) for TRA vs 2.8% (2796/98 730) for TFA; 1-year mortality was 4.6% (24 948/538 098) for TRA vs 9.5% (7536/79 416) for TFA. Adjusted analysis showed that TFA was significantly associated with higher mortality at both timepoints. The benefit of TRA was greatest in STEMI and NSTEMI but was also evident in elective cases and patients 80 years or older (Figure 2A and B).
PCI volumes and TRA/TFA ratio
TRA use varied by center (65% to 98%). High-volume and high-TRA centers showed a trend toward better outcomes, though differences were not statistically significant (Figure 3).
Discussion
This large, real-world study shows that TRA is associated with lower 30-day and 1-year mortality compared with TFA across a broad patient population. Our results align with prior randomized trials and support European Society of Cardiology (ESC) and American Heart Association/American College of Cardiology (AHA/ACC) guidelines. Notably, mortality benefits extended to elective cases and octogenarians. These findings argue for further expansion of TRA use.
Since 2018, ESC guidelines have recommended TRA as the default approach (Class I, Level A).9 The AHA/ACC adopted similar recommendations in 2021.10 Trials like RIVAL showed that TRA reduces vascular complications.4 RIFLE-STEACS, however, was the first to show a significant reduction in cardiac mortality and bleeding with TRA in patients with ST-elevation ACS.13 Lower bleeding rates and faster patient mobilization were suggested as key contributors to improved outcomes.14 The MATRIX (Minimizing Adverse Haemorrhagic Events by Transradial Access Site and Systemic Implementation of AngioX) trial also linked TRA to lower all-cause mortality and bleeding complications at 30 days in ACS patients.15 At the 1-year follow-up, net adverse clinical events remained lower in the TRA group.16
Despite these results, some authors have argued that procedural improvements (use of smaller sheaths, imaging puncture guidance, refined anticoagulation strategies) reduce TFA bleeding risks at the same extent as TRA.17 Indeed, the SAFARI-STEMI (Safety and Efficacy of Femoral Access versus Radial for Primary Percutaneous Intervention in ST-Elevation Myocardial Infarction) trial found no significant difference in 30-day mortality between TRA and TFA, but was underpowered because of early termination.7 Our study contradicts these claims, showing a significant short- and long-term mortality benefit of TRA, especially in ACS. Our findings are consistent with data from Hong Kong and SWEDEHEART registries, which reported better outcomes with TRA.18,19 Meta-analyses by Senguttuvan et al and Ando et al further reinforce the mortality benefits of TRA in ACS patients.20,21
Evidence for elective PCI is more limited. Some studies questioned TRA benefits in stable patients, but our data show significant mortality reduction at 30 days and 1 year.22
Octogenarians, a group traditionally associated with higher procedural risk, also benefited significantly; this aligns with previous studies suggesting TRA offers better survival outcomes and fewer complications in older patients.5,23,24
TRA adoption varies widely in the Netherlands, from 65% to 98%. This may reflect procedural complexity, operator preference, or experience. However, the mortality benefit appeared independent of center PCI volume or TRA/TFA ratio. Unlike trials that showed correlation between high TRA use and improved outcomes, our data show benefit across all levels of TRA use.4,15,25
Limitations
First, as an observational study, causality could not be established. In addition, residual confounding and selection bias, such as anticoagulation regimen, peripheral vascular disease, and frailty score, cannot be excluded. Moreover, the lack of bleeding complications and stent thrombosis limits mechanistic insight. In addition to bleeding complications, TRA might also reduce acute kidney injury, a hypothesis our dataset could not confirm.26 Finally, the exclusion of patients with cardiogenic shock or CTO restricts generalizability.
Conclusions
In real-life practice, TRA is associated with significantly better short- and long-term mortality outcomes than TFA. Our findings confirm those of previous randomized trials and support guideline recommendations for broad implementation of TRA for PCI.
Affiliations and Disclosures
Ioannis Karalis, MD, PhD1; Marijke JC Timmermans, PhD2; Andrea Tuccillo, MD3; J. Wouter Jukema, MD, PhD1,4; Lineke Derks, MSc2; Eva C. Verbeek, PhD3; Giovanni Amoroso, MD, PhD3; on behalf of the PCI Registration Committee of the Netherlands Heart Registration (NHR)
From the 1Leiden University Medical Center, Leiden, the Netherlands; 2Netherlands Heart Registration (NHR), Utrecht, the Netherlands; 3OLVG Amsterdam, Amsterdam, the Netherlands; 4Netherlands Heart Institute, Utrecht, the Netherlands.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Giovanni Amoroso, MD, PhD, Department of Cardiology, OLVG Amsterdam, Oosterpark 9, 1091 AC Amsterdam, the Netherlands. Email: g.amoroso@olvg.nl; X: @gioamor68; Instagram: @gioamor
References
1. Campeau L. Percutaneous radial artery approach for coronary angiography. Cathet Cardiovasc Diagn. 1989;16(1):3-7. doi:10.1002/ccd.181016010
2. Kiemeneij F, Laarman GJ. Percutaneous transradial artery approach for coronary stent implantation. Cathet Cardiovasc Diagn. 1993;30(2):173-178. doi:10.1002/ccd.1810300220
3. Campelo-Parada F, Carrié D, Bartorelli AL, et al; CENTURY II Investigators. Radial versus femoral approach for percutaneous coronary intervention: MACE outcomes at long-term follow-up. J Invasive Cardiol. 2018;30(7):262-268.
4. Jolly SS, Yusuf S, Cairns J, et al; RIVAL trial group. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011;377(9775):1409-1420. doi:10.1016/S0140-6736(11)60404-2
5. Lee HW, Cha KS, Ahn J, et al; Korea Acute Myocardial Infarction Registry Investigators. Comparison of transradial and transfemoral coronary intervention in octogenarians with acute myocardial infarction. Int J Cardiol. 2016;202:419-424. doi:10.1016/j.ijcard.2015.09.004
6. Mamas MA, Anderson SG, Ratib K, et al; British Cardiovascular Intervention Society; National Institute for Cardiovascular Outcomes Research. Arterial access site utilization in cardiogenic shock in the United Kingdom: is radial access feasible? Am Heart J. 2014;167(6):900-908.e1. doi:10.1016/j.ahj.2014.03.007
7. Le May M, Wells G, So D, et al. Safety and efficacy of femoral access vs radial access in ST-segment elevation myocardial infarction: The SAFARI-STEMI randomized clinical trial. JAMA Cardiol. 2020;5(2):126-134. doi:10.1001/jamacardio.2019.4852
8. Mason PJ, Shah B, Tamis-Holland JE, et al; American Heart Association Interventional Cardiovascular Care Committee of the Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Peripheral Vascular Disease; and Council on Genomic and Precision Medicine. An update on radial artery access and best practices for transradial coronary angiography and intervention in acute coronary syndrome: a scientific statement from the American Heart Association. Circ Cardiovasc Interv. 2018;11(9):e000035. doi:10.1161/HCV.0000000000000035
9. Neumann FJ, Sousa-Uva M, Ahlsson A, et al; ESC Scientific Document Group. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87-165. doi:10.1093/eurheartj/ehy394
10. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79:e21-e129. doi:10.1016/j.jacc.2021.09.006
11. Timmermans MJC, Houterman S, Daeter ED, et al; PCI Registration Committee of the Netherlands Heart Registration and the Cardiothoracic Surgery Registration Committee of the Netherlands Heart Registration. Using real-world data to monitor and improve quality of care in coronary artery disease: results from the Netherlands Heart Registration. Neth Heart J. 2022;30(12):546-556. doi:10.1007/s12471-022-01672-0
12. Houterman S, van Dullemen A, Versteegh M, et al; PCI Registration Committee of the Netherlands Heart Registration. Data quality and auditing within the Netherlands Heart Registration: using the PCI registry as an example. Neth Heart J. 2023;31(9):334-339. doi:10.1007/s12471-022-01752-1
13. Romagnoli E, Biondi-Zoccai G, Sciahbasi A, et al. Radial versus femoral randomized investigation in ST-segment elevation acute coronary syndrome: the RIFLE-STEACS (Radial Versus Femoral Randomized Investigation in ST-Elevation Acute Coronary Syndrome) study. J Am Coll Cardiol. 2012;60(24):2481-2489. doi:10.1016/j.jacc.2012.06.017
14. Vink MA, Amoroso G, Dirksen MT, et al. Routine use of the transradial approach in primary percutaneous coronary intervention: procedural aspects and outcomes in 2209 patients treated in a single high-volume centre. Heart. 2011;97(23):1938-1942. doi:10.1136/heartjnl-2011-300524
15. Valgimigli M, Gagnor A, Calabró P, et al; MATRIX Investigators. Radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: a randomised multicentre trial. Lancet. 2015;385(9986):2465-2476. doi:10.1016/S0140-6736(15)60292-6
16. Valgimigli M, Frigoli E, Leonardi S; MATRIX Investigators. Radial versus femoral access and bivalirudin versus unfractionated heparin in invasively managed patients with acute coronary syndrome (MATRIX): final 1-year results of a multicentre, randomised controlled trial. Lancet. 2018;392(10150):835-848. doi:10.1016/S0140-6736(18)31714-8
17. Marso SP, Amin AP, House JA, et al; National Cardiovascular Data Registry. Association between use of bleeding avoidance strategies and risk of periprocedural bleeding among patients undergoing percutaneous coronary intervention. JAMA. 2010;303(21):2156-2164. doi:10.1001/jama.2010.708
18. Ng AK, Ng PY, Ip A, Jim MH, Siu CW. Association between radial versus femoral access for percutaneous coronary intervention and long-term mortality. J Am Heart Assoc. 2021;10(15):e021256. doi:10.1161/JAHA.121.021256
19. Dworeck C, Redfors B, Völz S, et al. Radial artery access is associated with lower mortality in patients undergoing primary PCI: a report from the SWEDEHEART registry. Eur Heart J Acute Cardiovasc Care. 2020;9(4):323-332. doi:10.1177/2048872620908032
20. Senguttuvan NB, Reddy PMK, Shankar P, et al. Trans-radial approach versus trans-femoral approach in patients with acute coronary syndrome undergoing percutaneous coronary intervention: an updated meta-analysis of randomized controlled trials. PLoS ONE. 2022;17(4):e0266709. doi:10.1371/journal.pone.0266709
21. Andò G, Capodanno D. Radial versus femoral access in invasively managed patients with acute coronary syndrome: a systematic review and meta-analysis. Ann Intern Med. 2015;163(12):932-940. doi:10.7326/M15-1277
22. Gargiulo G, Giacoppo D, Jolly SS, et al; Radial Trialists’ Collaboration. Effects on mortality and major bleeding of radial versus femoral artery access for coronary angiography or percutaneous coronary intervention: meta-analysis of individual patient data from 7 multicenter randomized clinical trials. Circulation. 2022;146(18):1329-1343. doi:10.1161/CIRCULATIONAHA.122.061527
23. Hu F, Yang Y, Qiao S, et al. Comparison between radial and femoral approach for percutaneous coronary intervention in patients aged 80 years or older. J Interv Cardiol. 2012;25(5):513-517. doi:10.1111/j.1540-8183.2012.00732.x
24. Louvard Y, Benamer H, Garot P, et al; OCTOPLUS Study Group. Comparison of transradial and transfemoral approaches for coronary angiography and angioplasty in octogenarians (the OCTOPLUS study). Am J Cardiol. 2004;94(9):1177-1180. doi:10.1016/j.amjcard.2004.07.089
25. Adamo M, Byrne RA, Baumbach A, Haude M, Windecker S, Valgimigli M. Assessing the cardiology community position on transradial intervention and the use of bivalirudin in patients with acute coronary syndrome undergoing invasive management: results of an EAPCI survey. EuroIntervention. 2016;12(9):1154-1163. doi:10.4244/EIJY15M12_01
26. Wang C, Chen W, Yu M, Yang P. Comparison of acute kidney injury with radial vs. femoral access for patients undergoing coronary catheterization: an updated meta-analysis of 46,816 patients. Exp Ther Med. 2020;20(5):42. doi:10.3892/etm.2020.9170










