

Tendinitis Induced by Distal Radial Artery Pseudoaneurysm Following a Percutaneous Coronary Intervention
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
A 72-year-old man with coronary artery disease presented to our hospital with exertional angina. He was taking 5 mg of apixaban twice a day for atrial fibrillation.
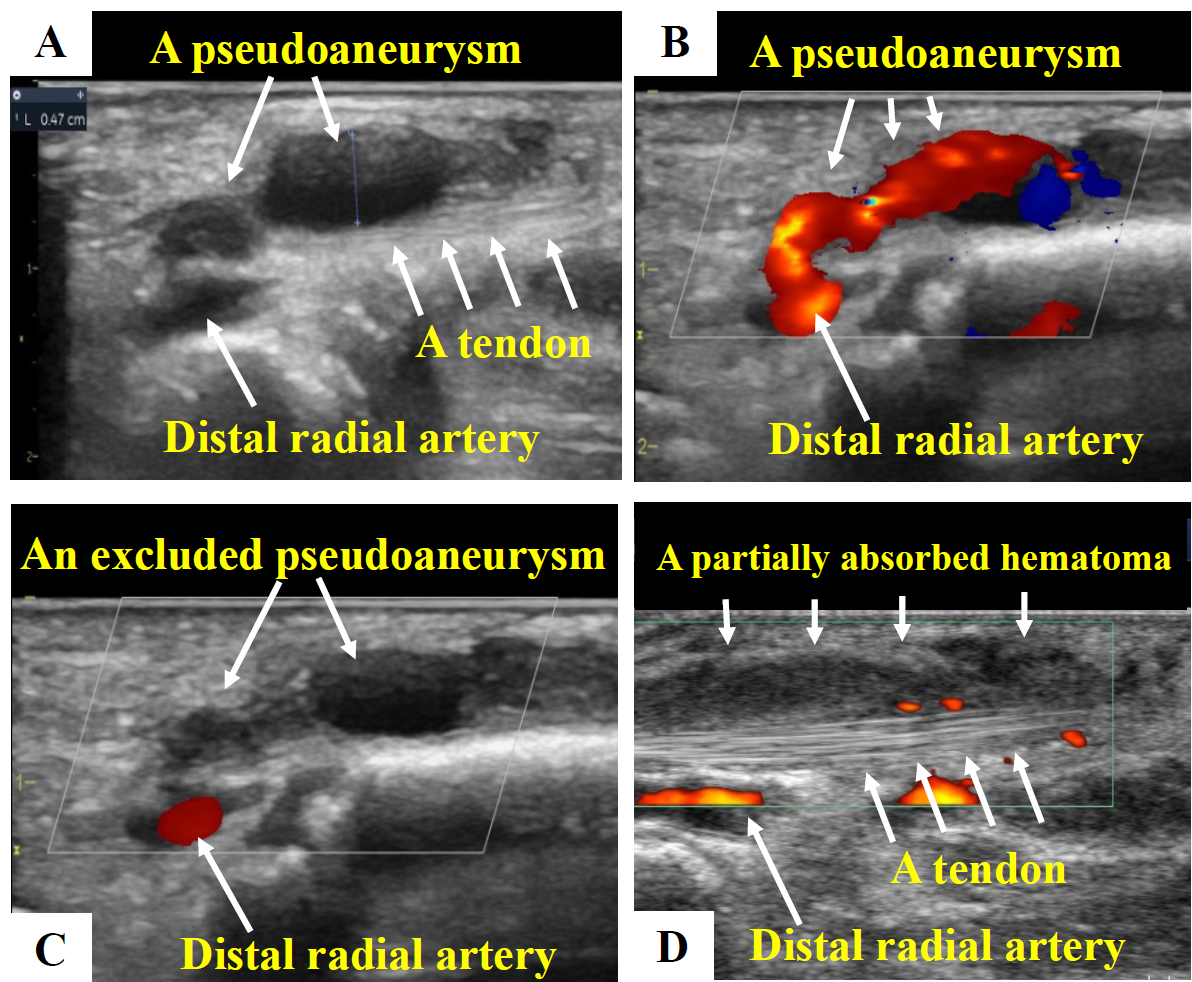
The patient underwent percutaneous coronary intervention for in-stent restenosis in the left anterior descending artery. Heparin (8000 units) and dual antiplatelet therapy with aspirin and prasugrel were administered. After the procedure, a 6F sheath was removed from the right distal radial artery, and a distal radial access-site compression device was placed. Although bleeding occurred 1 hour after the procedure, hemostasis was achieved by applying the device for 6 hours. However, 12 hours later, the patient started complaining of swelling and tenderness at the puncture site. An ultrasound test showed a hematoma with blood flowing into a pseudoaneurysm in the anatomic snuffbox (Figure A and B). Manual compression was performed with an ultrasound probe for approximately 3 hours, successfully excluding the pseudoaneurysm (Figure C).
Two weeks later, the patient presented with recurrent puncture-site pain. Ultrasound test showed resolution of the pseudoaneurysm; however, it demonstrated inflammatory changes around the right extensor pollicis longus tendon irritated by remnants of a partially absorbed hematoma, meeting the diagnosis of tendinitis (Figure D). After observation, his symptoms resolved spontaneously in a few months.
Pseudoaneurysm is a rare complication that occurs in less than 1% of distal radial artery access cases. The tendon of the right extensor pollicis longus crosses the anatomical snuffbox, which may be involved in the development of complications such as tendinitis. Local inflammation in the snuffbox due to the hemorrhagic complication is believed to have caused tendinitis in this case.
Affiliations and Disclosures
Tomohiro Fujisaki, MD, PhD; Shuichi Yoneda, MD, PhD; Yasuhide Asaumi, MD, PhD; Teruo Noguchi, MD, PhD
From the Department of Cardiovascular Medicine, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the information described in the manuscript and to the publication of the data, including any and all images.
Address for correspondence: Shuichi Yoneda, MD, PhD, Department of Cardiovascular Medicine, National Cerebral and Cardiovascular Center, 6-1 Kishibeshinmachi, Suita, Osaka 564-8565, Japan. Email: yonedashuichi1976@ncvc.go.jp
