

Micra Leadless Pacemaker Implantation via the Right Internal Jugular: Setup and Technique Insights
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
We present the first 2 Micra VR2 (Medtronic) implantations via the right internal jugular vein (RIJ) in Greece. This approach offers a direct, less tortuous route to the right ventricle, aiding catheter control and septal positioning.
Case 1 involved a 74-year-old woman with diabetes and morbid obesity who was referred for pace-and-ablate therapy for refractory atrial fibrillation. Ongoing lower limb infections rendered femoral access unfeasible. Case 2 was a 75-year-old woman with a mechanical mitral valve, prior embolism while on anticoagulation, and small body habitus, for whom transfemoral access posed thromboembolic and technical challenges.
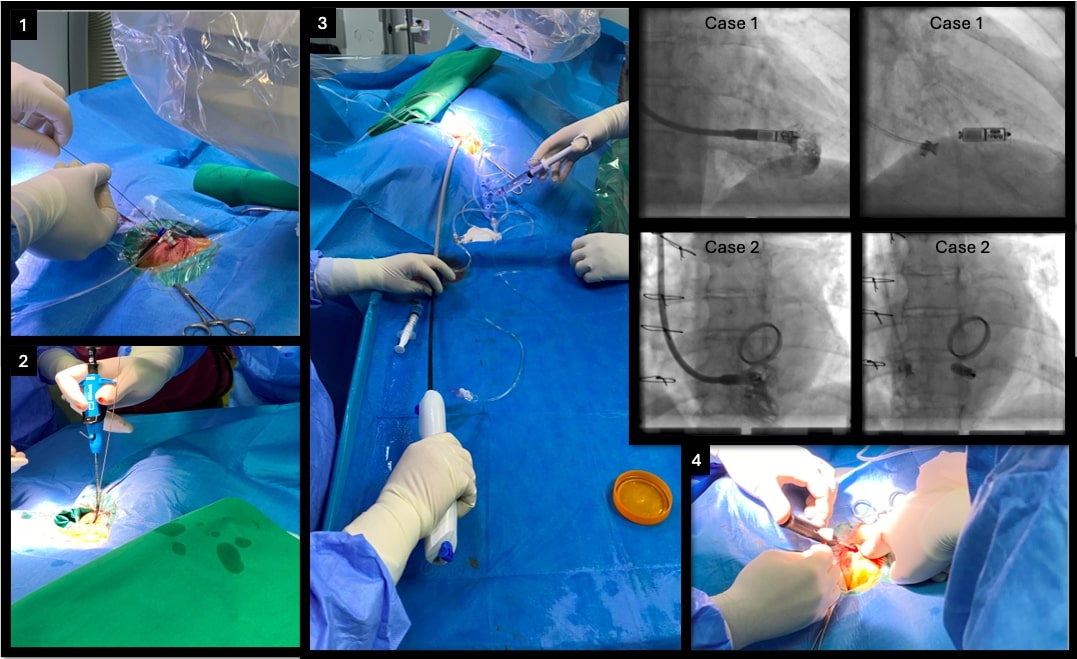
In both cases, the RIJ approach was deemed the only safe and feasible option. Procedures were performed under local anesthesia in the electrophysiology lab and were identical for both patients. Each was placed in the standard supine position with the C-arm rotated 90° leftward to allow right-neck access and facilitate manipulation of the Micra delivery system. Initial ultrasound confirmed a patent RIJ with a diameter greater than 1 cm. Ultrasound-guided puncture was performed, and a 6F sheath was inserted to secure access (Figure; panel 1). After placement of a 0.035-inch stiff guidewire, the sheath was removed, and 2 Perclose ProGlide sutures (Abbott) were deployed at 90° angles using the double preclose technique (Figure; panel 2). A 9F sheath was then inserted for superior vena cava venography, which confirmed unobstructed flow to the right atrium. Serial dilatation (14F to 18F) was performed, allowing safe advancement of the 27F Micra introducer sheath (Figure; panel 3). To minimize tip force, the Micra delivery system was advanced in a flexed configuration across the tricuspid valve. Under biplane fluoroscopy (RAO/LAO 45°), mid-septal positioning was confirmed (Figure; superimposed panels). Device deployment followed satisfactory electrical measurements. Fixation was confirmed by a pull-and-hold test, with at least 2 of 4 tines engaged. The tether was then cut, and the delivery system along with the sheath was withdrawn. Hemostasis was achieved using the pre-placed sutures (Figure; panel 4). The fluoroscopy times were 9.06 and 5.05 minutes with low radiation doses (air kerma: 134 mGy and 100 mGy) for each case, respectively. Both patients were mobilized immediately. No puncture site-related complications were seen.
The RIJ approach is a safe, feasible alternative for high-risk patients and may help expand leadless pacing to those with challenging anatomy or femoral access contraindications.
Affiliations and Disclosures
Maria Angelaki, MD, PhD; George Fotos, MD, MSc; Dimitrios Karelas, MD, MSc; Panagiota Manolakou, MD; Apostolos Christou, MD
From the Cardiology Department, Hellenic Red Cross Hospital Korgialenio-Benakio, Athens, Greece.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient(s) for the intervention(s) described in the manuscript and for the publication thereof, including any and all images.
Address for correspondence: Dimitrios Karelas, MD, MSc, Athanasaki 2, Athens, Greece. Email: dim.f.karelas@gmail.com
