

Excessive Force-Induced Eversion Endarterectomy on the Radial Artery Spasm: Uncontrolled Force Is Not Force
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
A 58-year-old woman presented with increasing exertional dyspnea and chest pain. She had a history of diabetes mellitus, hypertension, and a positive treadmill test result. Physical examination, echocardiography, and laboratory parameters were normal and suggested diagnostic coronary angiography. The left radial artery (RA) was cannulated using a 6F sheath, and she was given 2500 U heparin and 200 mcg nitroglycerine through the sheath.
By the left RA approach, there was difficulty advancing the 5F right diagnostic catheter under a 0.035-inch hydrophilic guidewire. While trying to advance or withdraw the catheter, the catheter could not be moved from the brachial region. The patient complained of intense pain and discomfort. Despite intra-arterial vasodilator agents (nicardipine 600 mcg and 800 mcg nitroglycerin), sedation (midazolam 4 mg and fentanyl 50 mcg), and external massage to the arm, the RA spasm did not resolve.
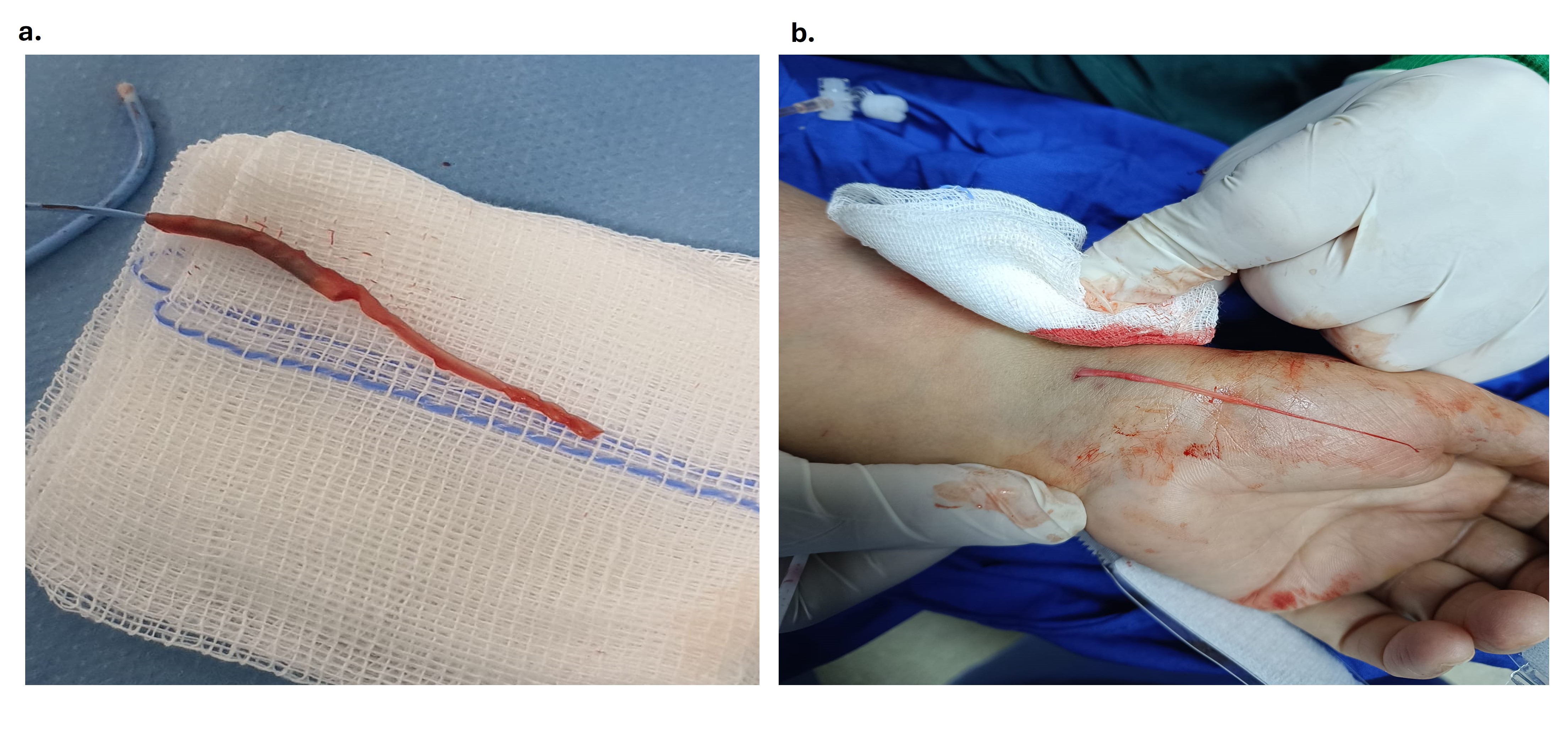
The catheter was left in the spasm area, and coronary angiography was performed via the right femoral arterial approach (Video). Noncritical coronary artery stenoses were detected, and medical follow-up was planned. After approximately 30 minutes, the patient was under sedation and the catheter in the spasm area was withdrawn with mild force. It was observed that the RA came out from the puncture site with the catheter, and the intima of the RA turned upside down in the form of an eversion endarterectomy (Figure A). The eversion endarterectomy portion extending from the radial puncture site was cut, and no bleeding or swelling was detected (Figure B). Elevation, pressure, cold application, and an analgesic agent were applied to the arm area. One day later, there was an obstructed blood flow with a suspicious thrombus image from the antecubital region to the distal punctured radial area on Doppler ultrasonography. The ulnar, brachial, and after-punctured distal RA segments were patent. No subcutaneous hematoma, hand ischemia, or any conditions requiring intervention were detected, and the patient was discharged asymptomatic.
Transradial arterial access for coronary angiography and interventions is increasing. RA spasm, RA thrombotic occlusion, and subcutaneous hematoma are common complications; however, active bleeding, compartment syndrome, RA dissection, perforation, avulsion, eversion, eversion endarterectomy, arteriovenous fistula, hand ischemia, and amputation may be other rare complications. There is no definitive consensus for the treatment of RA spasm. Vasodilators, spasmolytic cocktails, anxiolytics, sedation, analgesics, heat application to the spasm area, nerve block, and general anesthesia are recommended as applicable treatments. Excessive force and withdrawal should never be applied. Even if it takes a long time, spasm relief must be awaited patiently.
Affiliations and Disclosures
Murat Akcay, MD; Fuatcan Balaban, MD; Nisanur Danacı Kol, MD
From the Department of Cardiology, Faculty of Medicine, Ondokuz Mayis University, Samsun, Turkey.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: Written permission was obtained from the patient for publication of the case report.
Artificial intelligence (AI) statement: No AI-assisted technologies (such as large language models, chatbots, or image creators) were used in the production of submitted work.
Address for correspondence: Murat Akcay, MD, Department of Cardiology, Ondokuz Mayis University, Samsun, Turkey. Email: drmuratakcay@hotmail.com










