Endovascular Repair of a Complex Thoracoabdominal Aneurysm Using Thoracoabdominal Branch Endoprosthesis (TAMBE) in a High-Risk Vascular Patient
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
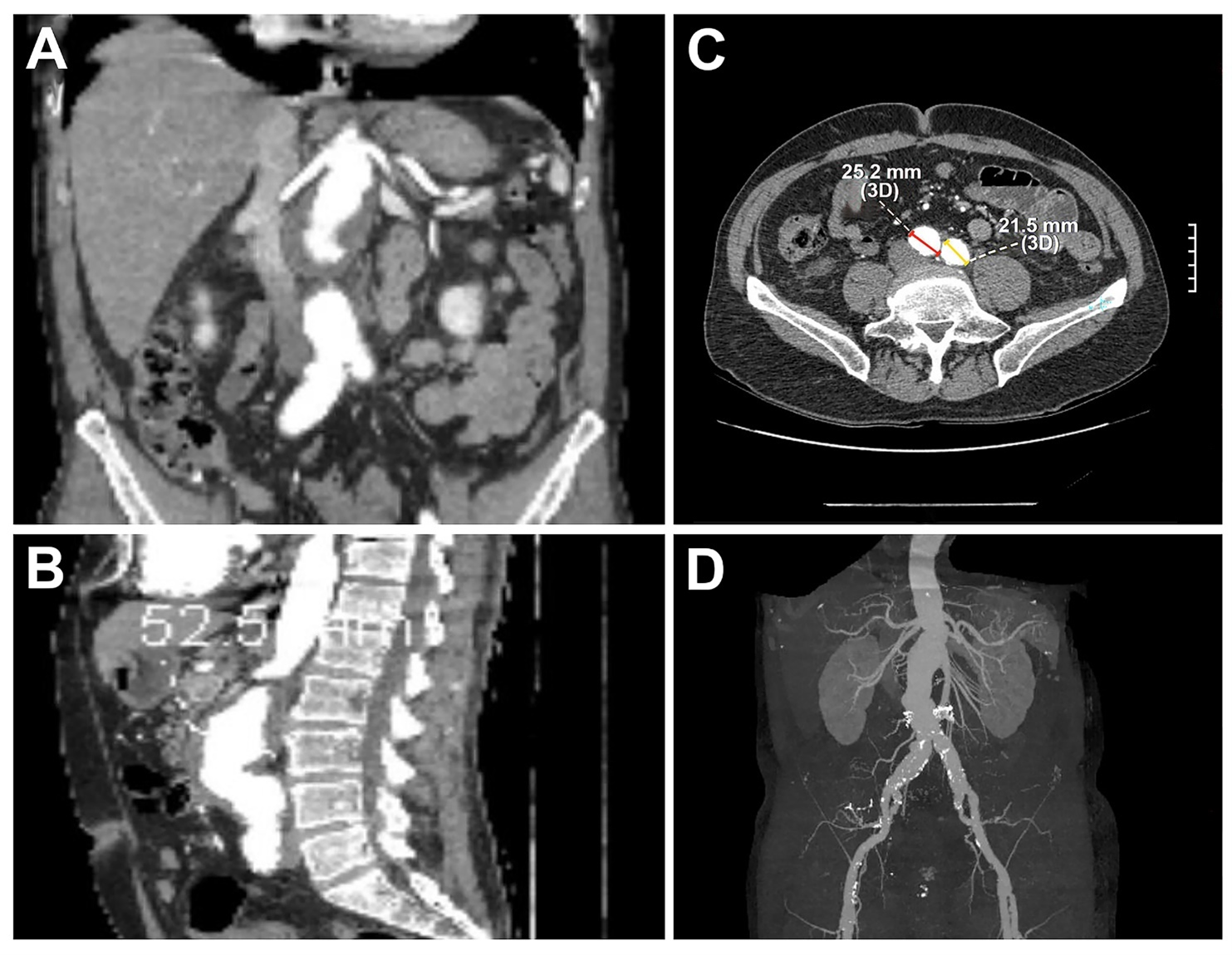
A 65-year-old man with a medical history of coronary artery disease (6 stents) and prior left femoral-popliteal bypass presented for routine abdominal aortic aneurysm (AAA) surveillance. Computed tomography angiography (CTA) demonstrated a 5.2-cm juxtarenal AA—a 5-mm increase over 6 months—along with bilateral common iliac aneurysms (Figures 1 and 2). Following a multidisciplinary evaluation, the patient was selected for treatment using the Thoracoabdominal Branch Endoprosthesis (TAMBE) device (W. L. Gore & Associates, Inc.).
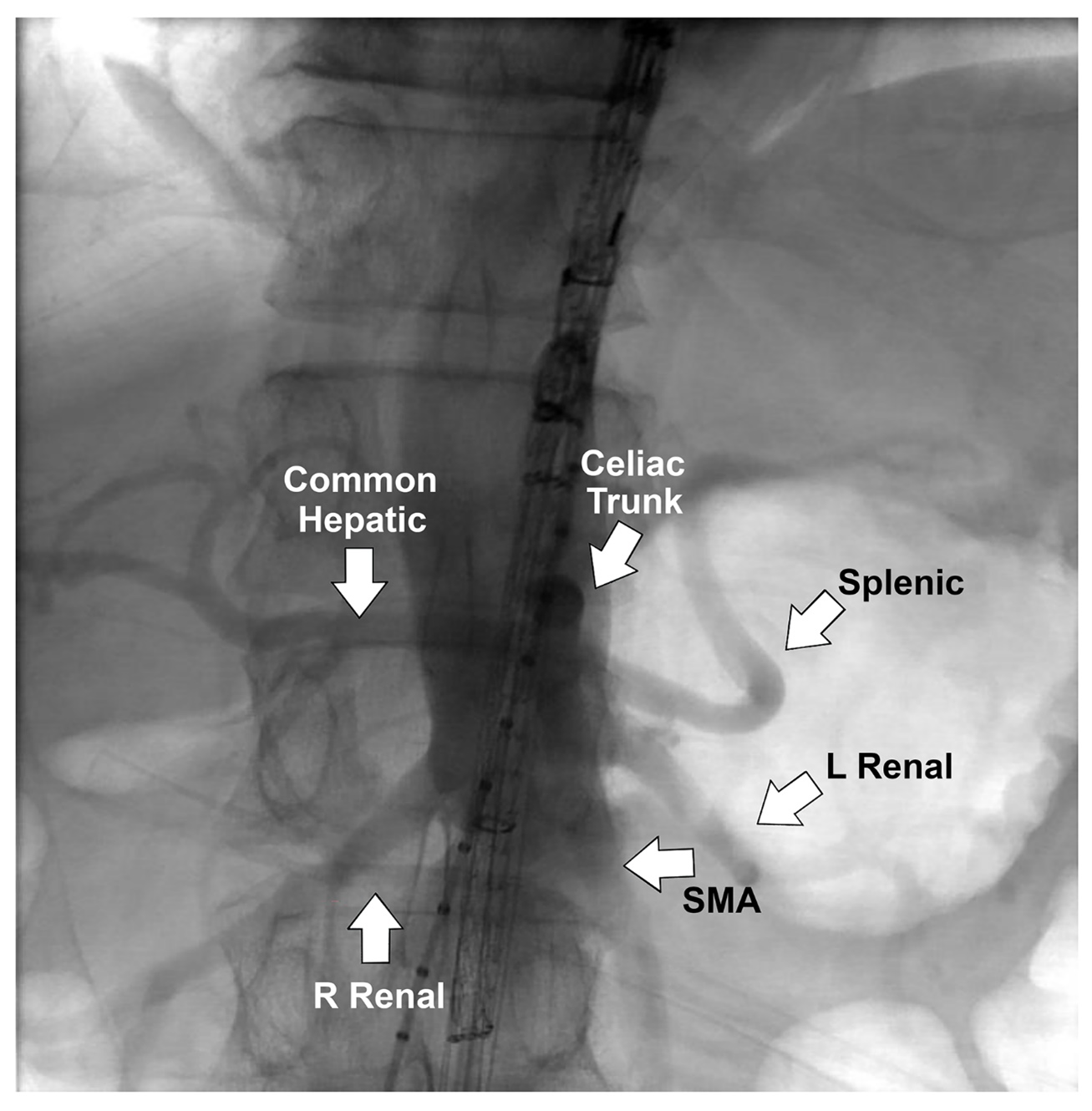
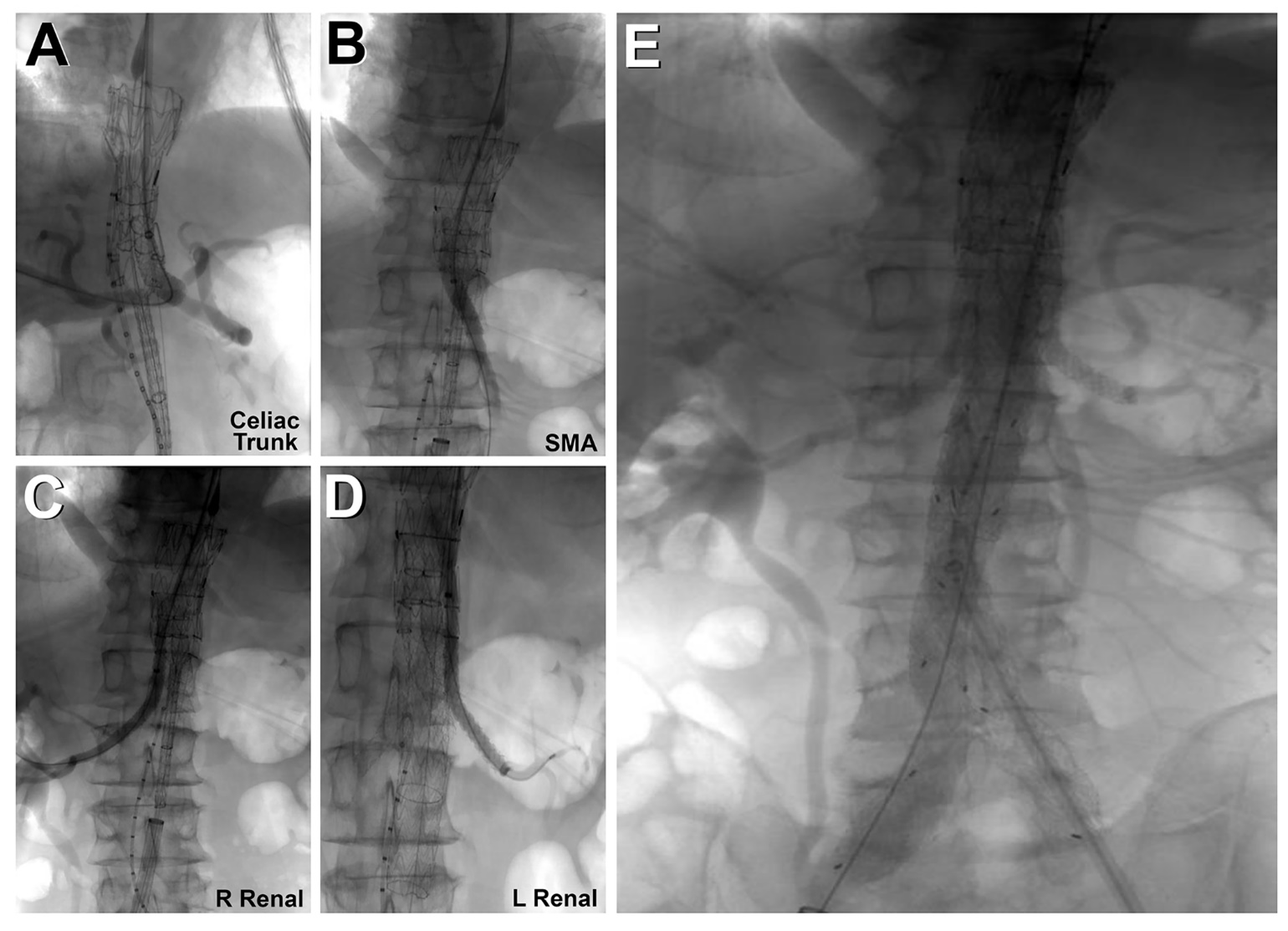
Both femoral arteries were accessed percutaneously with a Perclose device (Abbott). Left axillary artery cutdown was performed, and a 12F sheath was inserted; a 22F and a 12F sheath were deployed in the right and left femoral arteries, respectively. The TAMBE device was inserted from the right groin into the aorta and partly deployed. Using the axillary sheath, the celiac, superior mesenteric, and bilateral renal arteries were sequentially cannulated, and VIABAHN VBX stents (W. L. Gore & Associates, Inc.) were deployed. The infrarenal branch was deployed from the right groin into the TAMBE device, followed by ipsilateral limb extension from the right groin and the contralateral limb from the left groin.
CTA at completion confirmed complete exclusion of the aneurysm with preserved flow to the visceral and bilateral internal iliac arteries (Figure 3, Video 1). The total procedure time was 3 hours. The patient was discharged on the first postoperative day without complications. Two-week postoperative CTA (Video 2) confirmed patency of all target vessels and exclusion of the aneurysm sac without endoleak or migration.
Affiliations and Disclosures
Chaitanya Tumuluri, MBBS; M. Fuad Jan, MBBS (Hons), MD; Prabhjot Hundal, MD; Niloufar Javadi, MD; Rajeev Gupta, MD; Tanvir Bajwa, MD
From Aurora Cardiovascular and Thoracic Services, Aurora Sinai/Aurora St. Luke’s Medical Centers, Aurora Health Care, Milwaukee, Wisconsin.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient(s) for the intervention(s) described in the manuscript and for the publication thereof, including any and all images.
Address for correspondence: M. Fuad Jan, MBBS (Hons), MD, Aurora Cardiovascular and Thoracic Services, Aurora St. Luke’s Medical Center, 2801 W. Kinnickinnic River Parkway, Ste. 130, Milwaukee, WI 53215, USA. Email: Wi.publishing18@aah.org