

Aortic Dissection Presenting as Inferior Wall Myocardial Infarction
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
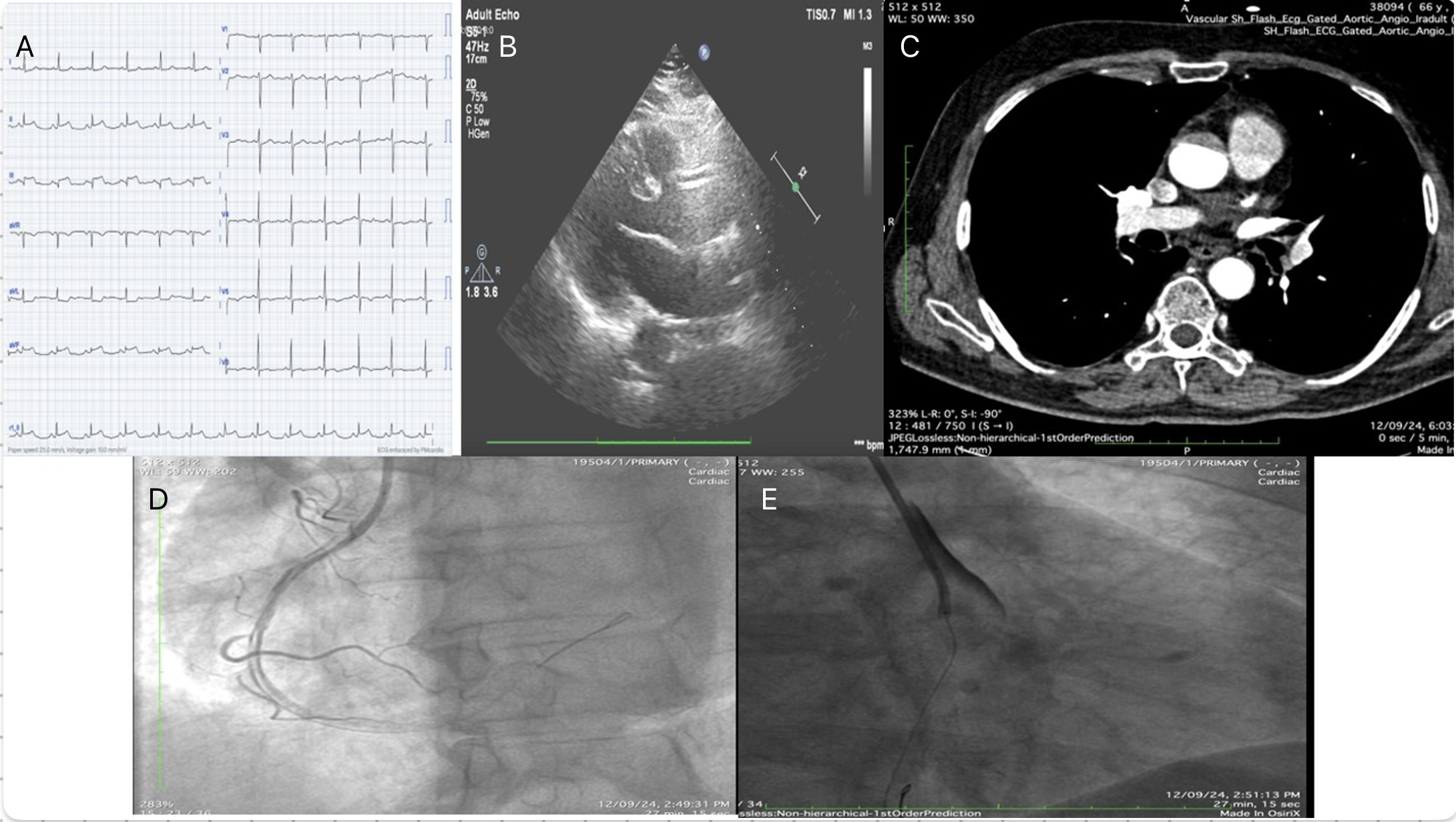
A 52-year-old man presented to the emergency department with chest pain and diaphoresis for the past 4 hours. The pain was maximum at onset, retrosternal, and radiating to his back. Upon admission, he was afebrile with a pulse rate of 70 beats per minute, respiratory rate of 20 breaths per minute, and blood pressure of 210/110 mm Hg. The patient had no prior history of hypertension, diabetes, or smoking. A 12-lead electrocardiogram (ECG) showed ST-segment elevation in the inferior leads with reciprocal changes in leads I and aVL, indicating an acute inferior wall myocardial infarction (Figure A). Screening transthoracic echocardiography was suggestive of inferior basal wall hypokinesia with an ejection fraction of 50%. The patient was taken for urgent coronary angiography, which revealed mild plaquing in the proximal left anterior descending artery and a 100% thrombotic cutoff of the ostia-proximal right coronary artery (RCA).
Given the diagnosis, the decision was made to proceed with angioplasty of the RCA. The RCA was successfully wired with a workhorse wire, and balloon inflation was performed at the site of the lesion. However, following balloon inflation, a spiral dissection of the artery was noted (Figure D). In response, an aortic angiogram was performed, which revealed a Type A aortic dissection (Figure E) and lead to the abandonment of the procedure.
Retrospectively, on a closer look at the echocardiogram, an intimal flap in the ascending aorta with acute aortic regurgitation was seen (Figure B). A computed tomography scan subsequently confirmed the presence of aortic dissection (Figure C), and the patient was immediately referred to cardiothoracic and vascular surgery where he underwent the Wheat procedure (aortic valve replacement with supra-coronary ascending aorta replacement) along with grafts to the RCA. He was subsequently discharged.
Affiliations and Disclosures
Lavina Chandwani, MD, DM; Anwar Hussain Ansari, MD, DM; Devesh Kumar, MD, MRCP, DM
From the Department of Cardiology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and for the publication of thereof, including photographs.
Address for correspondence: Devesh Kumar, MD, MRCP, DM, VMMC & Safdarjung Hospital, New Delhi 110029, India. Email: devesh2.dk@gmail.com
