


Simultaneous TAVI and EVAR in a High-Risk Patient With Severe Aortic Stenosis and Abdominal Aortic Aneurysm
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Mustafa Tunahan Öz, MD¹; Mohammed A.A. Alzawi²; Revan Israfilov1; Adnan Kaya, MD1,3
1Department of Cardiology, Bahçeşehir University Faculty of Medicine
2Bahçeşehir University Faculty of Medicine (Student)
3Professor of Cardiology, Dean of Bahçeşehir University Faculty of Medicine
Istanbul, Türkiye
Disclosures: The authors report no conflicts of interest regarding the content herein.
Patient Consent. Written informed consent was obtained from the patient for publication of this case and accompanying images.
The authors can be contacted via Mustafa Tunahan Öz, MD, at m.tunahanoz134@gmail.com
Abstract
Background. Severe aortic stenosis (AS) and abdominal aortic aneurysm (AAA) may coexist in elderly patients and pose significant therapeutic challenges, particularly in those with prohibitive surgical risk. Minimally invasive endovascular approaches, including transcatheter aortic valve implantation (TAVI) and endovascular aneurysm repair (EVAR), offer alternative treatment strategies.
Case Presentation. We describe a 78-year-old male with severe symptomatic AS and a 55-mm infrarenal AAA, along with multiple comorbidities including chronic obstructive pulmonary disease, reduced ejection fraction, advanced peripheral artery disease, and chronic kidney disease. Due to extremely high operative risk, the multidisciplinary heart team recommended a fully percutaneous approach. The patient underwent successful circumflex percutaneous coronary intervention, peripheral arterial revascularization, EVAR using an Endurant graft system (Medtronic) with CO₂ angiography, and transfemoral TAVI with a CoreValve Evolut R 29-mm bioprosthesis (Medtronic), performed sequentially in a single session under conscious sedation. The procedure was uneventful, and the patient was discharged on day three with no complications.
Conclusion. Simultaneous TAVI and EVAR represent a viable option for carefully selected high-risk patients with coexisting severe AS and AAA who are unsuitable for open surgery. This hybrid strategy minimizes anesthetic exposure, shortens hospitalization, and may reduce perioperative risk. Larger multicenter studies are needed to further refine patient selection and procedural sequencing.
Introduction
Severe aortic stenosis (AS) is a progressive and life-threatening valvular disease affecting up to 3% of adults over 65 years. In patients deemed unsuitable for open surgery, transcatheter aortic valve implantation (TAVI) has become the preferred therapeutic option.1
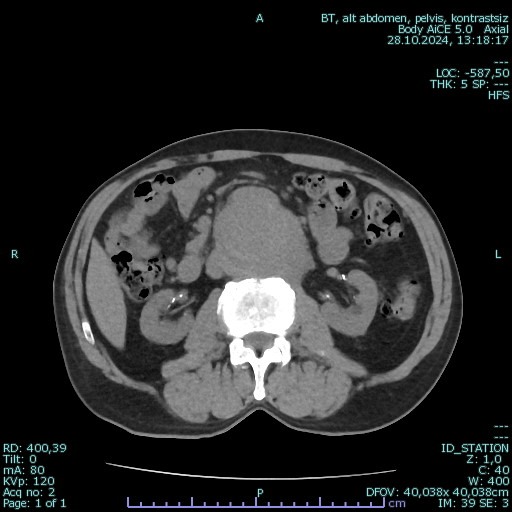
Abdominal aortic aneurysm (AAA), defined as an aortic diameter ≥30 mm, also presents commonly with advancing age.2 Once the aneurysm exceeds 55 mm, the risk of rupture increases significantly, making endovascular aneurysm repair (EVAR) the preferred modality for patients unfit for open repair (Figure 1).
The coexistence of severe AS and AAA introduces a clinical dilemma: both conditions independently carry high procedural risk, and traditional open surgery is generally contraindicated in frail individuals. Increasing evidence suggests that a combined, single-session TAVI–EVAR approach may be safe and effective in appropriately selected patients. Herein, we present a high-risk case managed successfully with a fully percutaneous hybrid intervention.
Case Presentation
A 78-year-old male with a medical history of atrial fibrillation, hypertension, hyperlipidemia, chronic kidney disease, and severe chronic obstructive pulmonary disease (COPD) presented with progressive lower-extremity claudication. Physical examination revealed stable vital signs and palpable femoral pulses. Electrocardiography showed atrial fibrillation. Transthoracic echocardiography demonstrated left ventricular ejection fraction of 40% with inferior wall hypokinesia and severe AS (mean gradient: 65 mmHg).
Carotid Doppler ultrasonography revealed advanced atherosclerotic disease (right carotid 78%, left carotid 70–80% stenosis). Coronary angiography showed total occlusion of the left anterior descending (LAD) coronary artery, severe circumflex stenosis (82–90%), and moderate right coronary artery (RCA) disease.
Computed tomography angiography revealed an infrarenal AAA measuring 55 mm with adequate proximal neck morphology and minimal mural thrombus.
Heart Team Decision
Given the patient’s severe COPD, reduced ejection fraction, extensive vascular disease, and elevated perioperative mortality risk, the heart team recommended a staged-in-one-session fully percutaneous strategy:
1. Percutaneous coronary intervention of the circumflex artery;
2. Peripheral revascularization: right superficial femoral artery (SFA) chronic total occlusion (CTO) recanalization, and left SFA balloon angioplasty;
3. EVAR using an Endurant stent graft system performed with CO₂ angiography to avoid contrast-induced nephropathy;
4. TAVI via transfemoral access with deployment of a CoreValve Evolut R 29 mm prosthesis.
Supplementary Video. CO₂ angiography demonstrating abdominal aortic anatomy prior to endovascular aneurysm repair in a high-risk patient with severe renal dysfunction.
Given the large infrarenal aneurysm and the need to advance large-bore transfemoral devices for TAVI, the heart team decided to perform EVAR first followed by TAVI in the same session, in order to stabilize the aneurysm and reduce the theoretical risk of aneurysm rupture or wall stress during manipulation of the valve delivery system.
Both femoral arteries were accessed with large-bore sheaths, and the entire intervention was performed under conscious sedation. No intra- or postoperative complications occurred. The patient was discharged on postoperative day three with stable renal function and marked symptomatic improvement.3
Discussion
Patients with concurrent severe AS and AAA represent a complex treatment population due to competing hemodynamic and anatomical risks.4 Traditional open surgical repair carries substantial morbidity, often rendering patients ineligible for standard procedures. In such cases, combining TAVI and EVAR within a single session provides several theoretical and practical advantages:
• Avoiding hemodynamic collapse: Repairing the AAA first may provoke acute afterload shifts in the presence of untreated AS, whereas delaying AAA repair after isolated TAVI may expose the patient to rupture risk.
• Minimized anesthesia exposure: Conscious sedation prevents pulmonary complications, particularly in COPD and frail, elderly patients.
• Single vascular access session: Reduces bleeding and access-related complications.5
• Early recovery and reduced hospital stay.
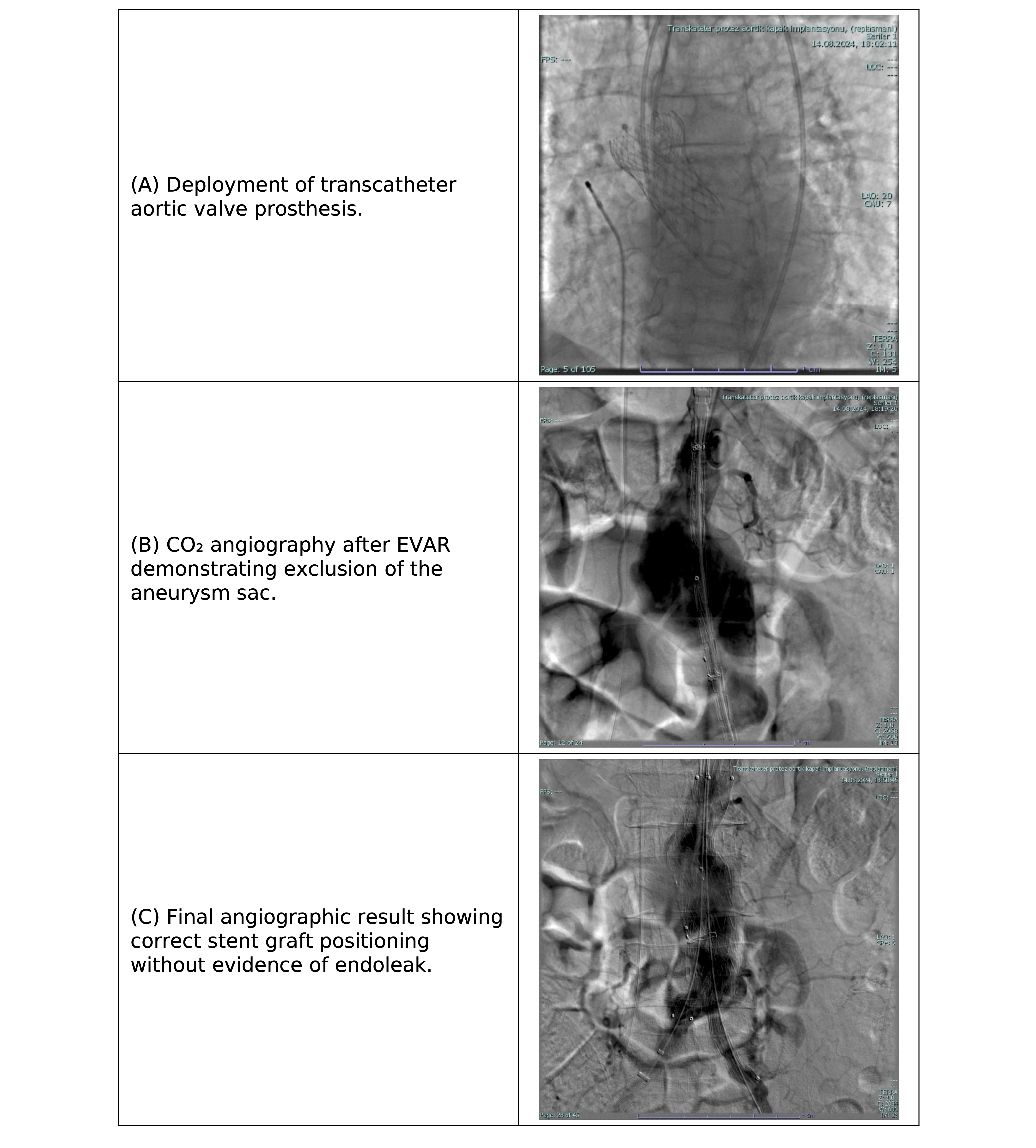
Emerging data from multicenter series support the safety of simultaneous TAVI–EVAR, with low perioperative complication rates in experienced centers (Figure 2).4
Procedure Sequencing
Some authors recommend performing EVAR before TAVI to avoid potential mechanical displacement of the aortic stent graft by stiff transcatheter valve delivery systems. However, both procedural sequences have been reported in the literature, and the optimal strategy should be individualized based on patient anatomy, vascular access conditions, and operator experience.6,7
Use of CO₂ Angiography
In this patient with chronic kidney disease, CO₂ angiography was beneficial in minimizing contrast-induced nephropathy while maintaining procedural accuracy.8
This case contributes to the growing evidence that combined endovascular approaches are feasible in high-risk cohorts and should be considered when open surgery is contraindicated.
Conclusion
Simultaneous TAVI and EVAR can be performed safely in highly selected patients with severe AS and AAA who are unsuitable for open surgery. A multidisciplinary strategy, careful anatomical evaluation, and experienced operators are critical for procedural success. Further multicenter data are needed to strengthen evidence and refine patient selection algorithms.
References
1. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021 Feb 2; 143(5): e72-e227. doi:10.1161/CIR.0000000000000923
2. Haque K, Bhargava P. Abdominal aortic aneurysm. Am Fam Physician. 2022 Aug; 106(2): 165-172.
3. Koutsias S, Karaolanis GI, Papafaklis MI, et al. Simultaneous transcatheter aortic valve implantation and infrarenal aortic aneurysm repair for severe aortic stenosis and abdominal aortic aneurysm: report of 2 cases and literature review. Vasc Endovascular Surg. 2020 Aug; 54(6): 544-548. doi:10.1177/1538574420927864
4. Gallitto E, Spath P, Faggioli GL, et al; Italian Multicenter T/EVAR + TAVI Studys Group. Simultaneous versus staged approach in transcatheter aortic valve implantation for severe stenosis and endovascular aortic repair for thoracic and abdominal aortic aneurysm. Eur J Cardiothorac Surg. 2024 Nov 4; 66(5): ezae379. doi:10.1093/ejcts/ezae379
5. Marchi F, Cerillo AG, Rizza A, et al. Large abdominal aortic aneurysm in a high-risk surgical patient: combined percutaneous transfemoral TAVI and EVAR procedure. J Heart Valve Dis. 2015 May; 24(3): 310-312.
6. Tan C, Weng JY, Gou ZS, et al. One-stop TEVAR and TAVR procedure for severe aortic stenosis with aortic arch aneurysm. JACC Case Rep. 2025 May 14; 30(10): 103922. doi:10.1016/j.jaccas.2025.103922
7. Sanoussi A, Aminian A, Abi-Khalil J. One-stop transcatheter aortic valve replacement and fenestrated endovascular aortic aneurysm repair: A case report. Radiol Case Rep. 2024 Jan 4; 19(3): 1162-1165. doi:10.1016/j.radcr.2023.12.041
8. Lee SR, Ali S, Cardella J, et al. Carbon dioxide angiography during peripheral vascular interventions is associated with decreased cardiac and renal complications in patients with chronic kidney disease. J Vasc Surg. 2023 Jul; 78(1): 201-208. doi:10.1016/j.jvs.2023.03.029


