

Billing and Coding for Total Ankle Replacement Surgery
Author Disclaimer: Case scenarios and suggested billing and coding depend on patient pathology, what was performed, and documentation. Use of modifiers and CPT are at the discretion of the surgeon. Please check individual insurance contracts. CPT codes are a registered trademark of the American Medical Association.
As total ankle arthroplasty expands to address increasingly complex deformities, surgeons must navigate strict NCCI edits and bundling rules to ensure accurate coding and reimbursement. Understanding when adjunct procedures are separately reportable—and documenting them correctly—is essential to avoiding denials.
Key Takeaways
· NCCI edits drive coding decisions: Surgeons must understand “separate procedure” designations and comprehensive code rules to avoid unintentional unbundling or denied claims.
· Adjunct procedures may be billable—but only with clear justification: Fixation, syndesmotic repair, osteotomies, and fusions can be separately coded when performed for distinct pathology and not as part of the total ankle surgical approach.
· Documentation is critical to reimbursement: Detailed operative reports that clearly distinguish pathology, surgical intent, and sequencing are essential to support appropriate CPT code selection in complex total ankle cases.
As technology has evolved, surgeons are able to perform total ankle arthroplasty procedures on varying degrees of deformities. With the advancement of this technology, indications and imaging criteria for total ankle replacement surgery have also expanded. A lot of time and effort goes into these cases intraoperatively. Billing and coding accordingly is necessary to ensure appropriate reimbursement for this time and effort; however, some surgeons are seeing denials as procedures are being “bundled” with the total ankle Current Procedural Terminology (CPT®) code.
Before surgeons can appropriately choose CPT codes, there are several important rules and regulations known as the National Correction Coding Initiative (NCCI) edits that physicians should be aware of.
The first edit involves CPT codes that have the designation “separate procedure.” The edit reads as follows1,2:
“If a CPT code descriptor includes the term “separate procedure,” the CPT code may not be reported separately with a related procedure. CMS interprets this designation to prohibit the separate reporting of a “separate procedure” when performed with another procedure in an anatomically related region often through the same skin incision, orifice, or surgical approach.”
Other important edits include excerpts from Chapter 1 of the manual including1,2:
- “Procedures shall be reported with the most comprehensive CPT code that describes the services performed;” and
- “A provider/supplier shall not report multiple HCPCS/CPT codes when a single comprehensive HCPCS/CPT code describes these services”
These presented edits are not all inclusive and I recommend each practitioner read the NCCI manual, particularly chapters 1 and 4.
Below, we present several example total ankle arthroplasty cases that inspire discussion on coding choices.

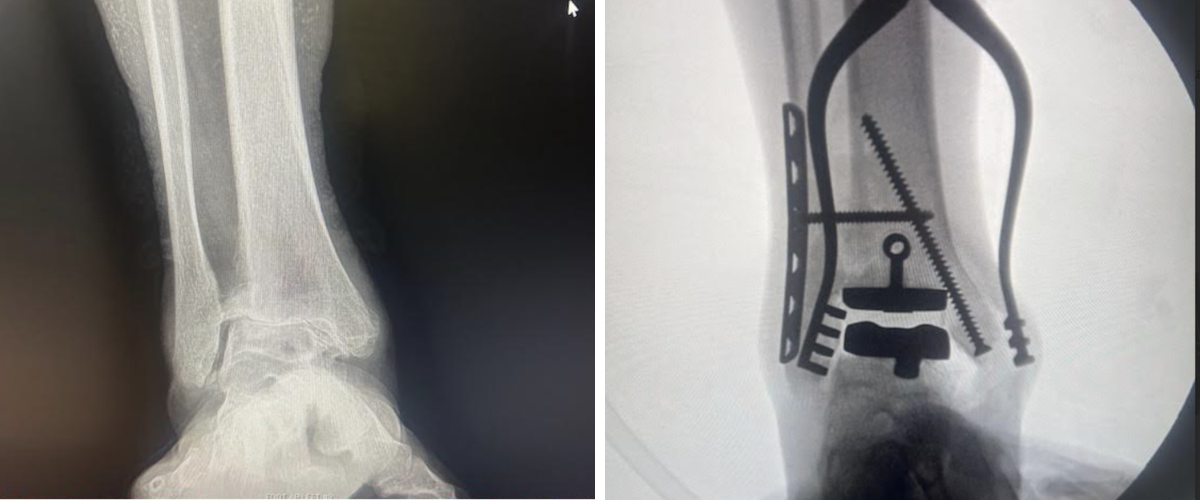
Case 1. This case demonstrates a staged total ankle replacement where the patient underwent a medial column fusion in a previous surgery. This date of service focused on just the ankle replacement, but as evidenced by the anteroposterior (AP) X-ray, there was a screw placed in the medial malleolus. I have often seen debate on how and if this is a codable procedure. Two CPT codes exist for this scenario; “open reduction internal fixation of medial malleolus fracture” versus “prophylactic treatment (nailing, pinning, plating or wiring) with or without methylmethacrylate, tibia.”3
Their uses are circumstantial. If a tibial tray cut causes a fracture or weakens the bone, prompting use of either code, the resulting pinning or fixation may be considered included in the total ankle arthroplasty code. However, if the fracture pre-existed, then it could be completely appropriate to fix the fracture separately from the total ankle procedure. In my opinion, the prophylactic pinning of tibia code is more appropriate in most scenarios. Often physicians feel this is a code for tumor resection, and certainly that is one indication; however, listed allowable ICD-10 codes for that CPT also include stress fracture, osteoporosis, and other disorders of continuity of bone, tibia.3 If the physician places the medial malleolus fixation first, prior to the total ankle procedure, due to other conditions, then it may, in my experience, be perfectly reasonable to bill that code.
Case 2. This case features an old syndesmotic injury as depicted in the preoperative films. Reduction of the syndesmosis is necessary for total ankle arthroplasty and is not included in the total ankle arthroplasty CPT.3 Therefore, in this instance, coding the open treatment of a distal tibiofibular joint (syndesmosis) disruption CPT code is appropriate. It is my opinion that dictation documentation is important here. The physician should clearly indicate in the operative report the presence of the syndesmosis injury, instability, etc and document how the repair took place separately from the total ankle arthroplasty. Again in this example one can note fixation in the medial malleolus and the same argument as in Case 1 above applies here.

Case 3. This next case depicts a large valgus deformity with a shortened fibula. The surgeon addressed the flatfoot deformity first before a staged total ankle procedure. Because of the fibula shortening and rotation, an osteotomy was necessary to regain length. Again, this procedure was performed due to anatomic and pathologic insufficiency and not as part of the total ankle replacement. It is appropriate here to code for the fibular osteotomy. This can be a complicated consideration in total ankle systems that require a fibula cut/take down to put in the total ankle implant. In thse cases, the osteotomy could be considered part of the total ankle because it is inherent within the surgical approach to the total ankle arthroplasty.

Case 4. This case depicts a flatfoot reconstruction with a total ankle arthroplasty. The flatfoot deformity required fusion of the entire medial column. It is important to distinguish between the fusion codes and pick appropriately. There are codes for arthrodesis, midtarsal or tarsometatarsal, single joint; Arthrodesis, midtarsal or tarsometatarsal, multiple or transverse; and Arthrodesis, midtarsal or tarsometatarsal, multiple or transverse; with osteotomy (eg, flatfoot correction).3 In this case, there was fusion of the first tarsometatarsal joint, the navicular-cuneiform joint and the talonavicular joint, and therefore one should use one of the multiple joint fusion codes. It is inappropriate to bill the single fusion code multiple times since a code exists for a multiple joint fusion.
Because of the severe flatfoot deformity, the surgeon made an osteotomy to realign the medial column. In this case, the best selection is the arthrodesis tarsometatarsal/midtarsal with osteotomy code. It should be noted that there is another code, “Arthrodesis, with tendon lengthening and advancement, midtarsal, tarsal navicular-cuneiform (eg: Miller type procedure).”3 If the surgeon does a lengthening or advancement of the tibialis posterior tendon, then this code should be selected. It would be inappropriate to use the multiple arthrodesis code and a separate tendon code since one code exists that describes the procedure. Choosing both would thus be unbundling. The talonavicular joint arthrodesis is included in the above codes and should not be coded separately.3
A posterior muscle group lengthening was necessary with this case as well. There are different codes depending on the level of lengthening with the gastrocnemius release having a different CPT code than that for the Achilles tendon lengthening. The CPT code for an Achilles lengthening is described as, “Lengthening or shortening of tendon, leg or ankle; single tendon (separate procedure).”3 This code has the (separate procedure) designation as described previously. I have observed some colleagues seeing this code not being paid secondary to this separate procedure designation. Surgeons should be aware of this, as well as the spectrum of codes available, and again be sure to pick the most appropriate code for what was performed. Other codes include, “Lengthening or shortening of tendon, leg or ankle; multiple tendons (through same incision),” and “Arthrotomy, posterior capsular release, ankle, with or without Achilles tendon lengthening.” These codes do not have the separate procedure designation and, at times, may more accurately reflect the procedures performed during a flatfoot reconstruction with a total ankle arthroplasty.

In Conclusion
Total ankle arthroplasty cases are often multifaceted with several other adjunct procedures performed. Properly and compliantly coding these cases is important to receive, and keep, full reimbursement for the time and skill that is involved. Remember, proper documentation and dictation in the operative report is vital to successful reimbursement.
Dr. Butto is currently employed at University Hospitals in Cleveland, OH, where she is actively involved in the teaching faculty of both the residency and the fellowship. In addition, she is also a Certified Professional Coder.
Dr. Flynn is a board-certified, fellowship trained podiatrist specializing in foot and reconstructive rearfoot and ankle surgery at Arizona Foot Health in Phoenix, Arizona.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.
All information regarding reimbursement, legislation, regulations, policy, and legal proceedings, is provided as a service to our audience. Commercially reasonable efforts have been made to ensure the accuracy of the information within this resource but HMP Global, their employees, their affiliates, contributors, commenters, and reviewers do not represent, guarantee, or warranty that any information provided within this resource is error-free. HMP Global, their employees, their affiliates, contributors, and reviewers disclaim all liability attributable to the use of any information, guidance, or advice contained in this resource. The responsibility for verifying information accuracy for individual use and in individual circumstances lies solely with the audience member. The information in this resource is also not a substitute for legal, medical, or business advice, and is for educational purposes only. Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Current Procedural Terminology is a Registered Trademark of the American Medical Association. CPT codes, descriptions and other data only are copyright 2025 American Medical Association. All rights reserved.
- Centers for Medicare & Medicaid Services. Chapter IV: Surgery: Musculoskeletal System. National Correct Coding Initiative Medicare Policy Manual. Revision date January 1, 2025. Published 2025. Accessed February 2, 2026. https://www.cms.gov/files/document/04-chapter4-ncci-medicare-policy-manual-2025finalcleanpdf.pdf
- Centers for Medicare & Medicaid Services. Medicare National Correct Coding Initiative (NCCI) Policy Manual for Medicare Services — All Chapters. Effective January 1, 2026. Published 2025. Accessed February 2, 2026. https://www.cms.gov/files/document/2026-ncci-medicare-policy-manual-all-chapters.pdf
- American Medical Association. Current Procedural Terminology: CPT® 2026 Professional Edition. 1st ed. American Medical Association; 2025.





