Using Photon-Counting CT to Image Stents in PCI Patients
Images/courtesy WellSpan Heart & Vascular Institute
Images/courtesy WellSpan Heart & Vascular Institute
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Images/courtesy WellSpan Heart & Vascular Institute
Percutaneous coronary intervention (PCI) with metallic stents is the mainstay of revascularization for patients who present with angina where coronary artery bypass surgery is not indicated. Partial volume artifacts and blooming present challenges to imaging these stents with coronary computed tomography angiography (CCTA). Photon-counting CT, with its enhanced spatial resolution and improved signal-to-noise ratio, may help alleviate these challenges.
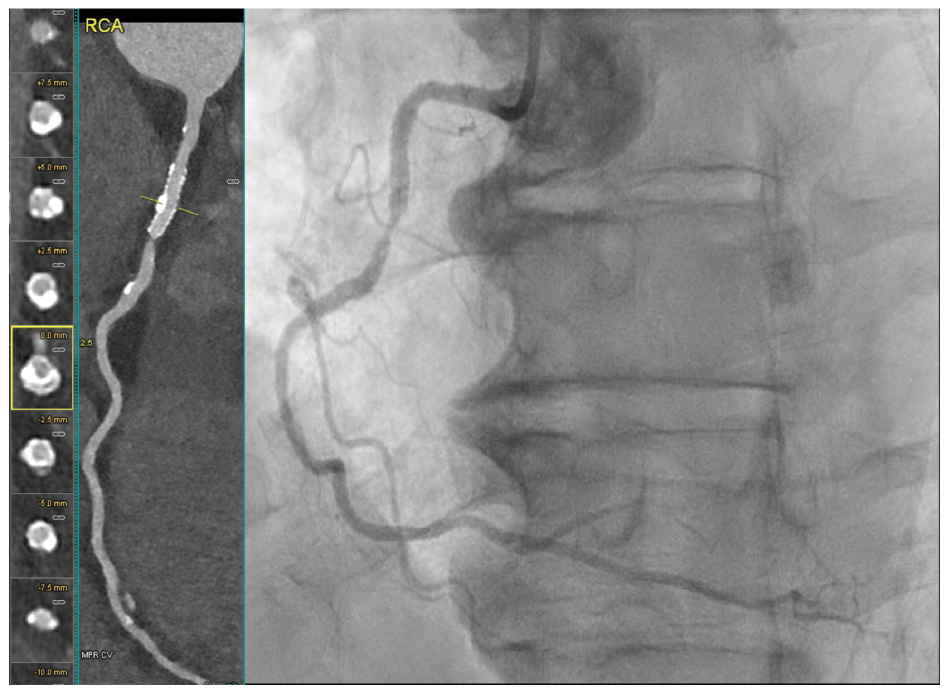
In this case, a 73-year-old male with a remote PCI to the right coronary artery (RCA) and circumflex coronary artery (Cx), dyslipidemia, and hypertension presented with chest discomfort on exertion. A CCTA (Naeotom Alpha PCCT scanner, Siemens Healthineers) was performed to evaluate the patient’s symptoms. Sharper kernels with higher iterative reconstruction were used to facilitate stent visualization. The CCTA demonstrated complex calcified and noncalcified plaque in the mid-segment of the left anterior descending (LAD) coronary artery (Figure 1) with moderate stenosis.
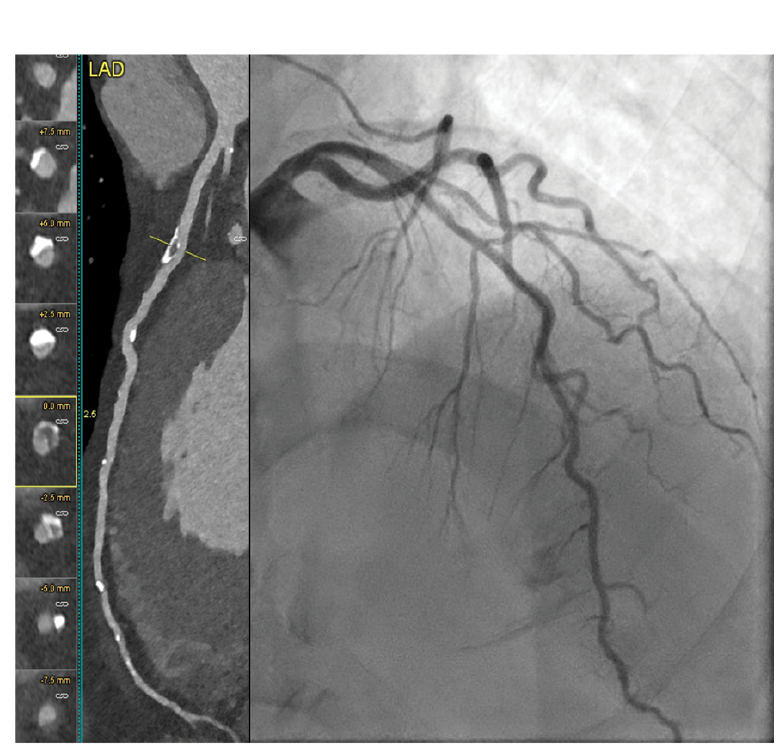
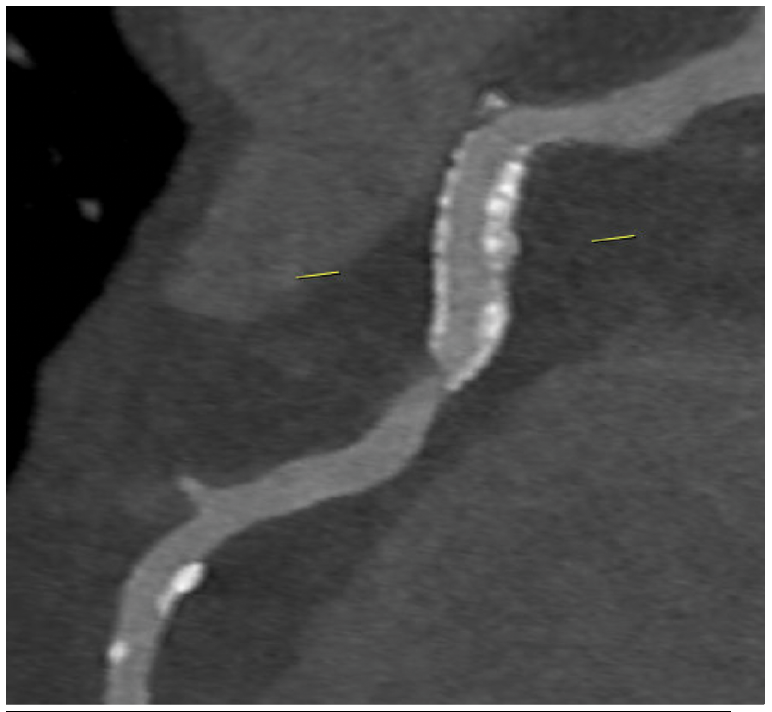
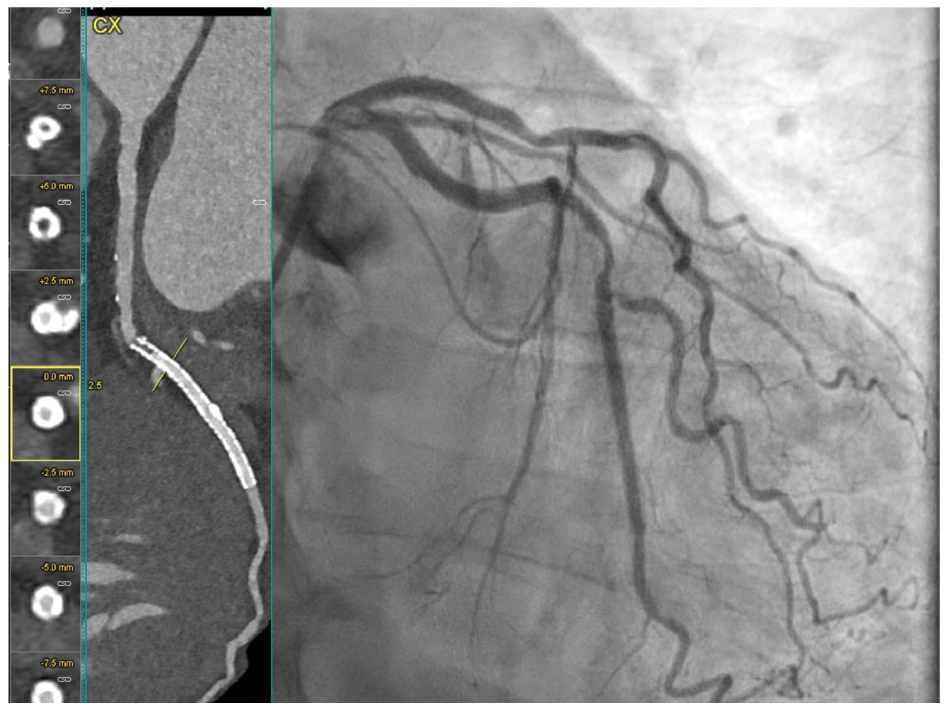
The RCA (Figure 2) demonstrated a patent stent but severe stenosis in the native artery (Figure 3) at the stent’s distal segment. Severe stenosis was noted in the Cx (Figure 4) proximal to the previously placed stent. CCTA findings were confirmed by invasive angiography. A diastolic hyperemia-free ratio (DFR) across the lesion in the LAD was abnormal at 0.89. The patient later received intravascular ultrasound-guided PCI of the Cx, LAD, and RCA.