Eventration of the Diaphragm Presenting as Unstable Angina: The Importance of Looking at Non-Cardiac Findings on Catheterization Cines
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Saiyeda S. Ali, MD1; Greeshma Molugu, MD2; Ruben Abreu, MD3; Asad Rizvi, MD3; Mehdi Khalafi, MD4
1Wayne State School of Medicine, Detroit, Michigan; 2PGY-3, Internal Medicine Residency Program, Medical City Fort Worth, Fort Worth, Texas;
3Cardiology Fellow, Cardiovascular Diseases Fellowship Program, Medical City Fort Worth, Fort Worth, Texas; 4Interventional Cardiologist, Medical City Fort Worth, Fort Worth, Texas
The authors can be contacted via Asad Rizvi, MD, at Asad.Rizvi@MedicalCityHealth.com.
Click here for a PDF of this article, courtesy of Cath Lab Digest.
Case Presentation
A 56-year-old male with a past medical history of gastroesophageal reflux disease and tobacco abuse presented to the emergency department with a chief complaint of chest pain and progressive shortness of breath of a year duration. The patient described pressure-like chest pain, located in the left precordial area, intermittent, and worse with exertion. Over the past few days, he experienced his symptoms even at rest. Pain was alleviated with sublingual nitroglycerin and rest. Over the last month, dyspnea on exertion had progressively worsened to the point that he was unable to perform his activities of daily living. The patient denied any similar presentation in the past.
He had been a smoker since he was 9 years old and drank 2-3 beers daily. He has a strong family history of premature coronary artery disease (CAD). He reported that he engaged in bull riding as a hobby, with multiple previous injuries from riding bulls. Upon arrival to the hospital, vital signs and physical exam were unremarkable. An electrocardiogram showed normal sinus rhythm without any ST changes. Lipid panel showed an LDL of 196 mg/dL, and other labs including CBC, CMP, troponin, BNP, and A1C were unremarkable.
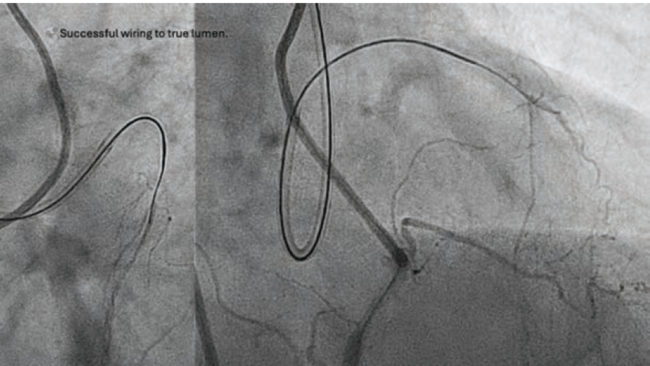
Video. Prominent elevation of the left diaphragm was seen on multiple cine views with bowel visualization above the heart.
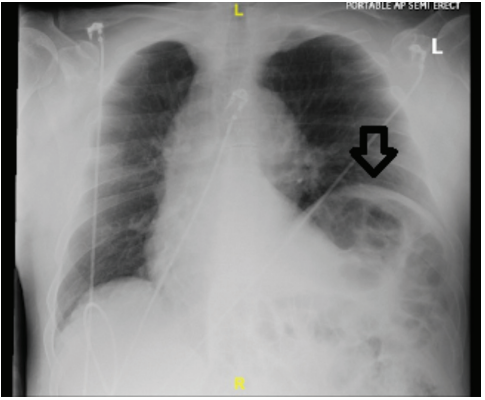
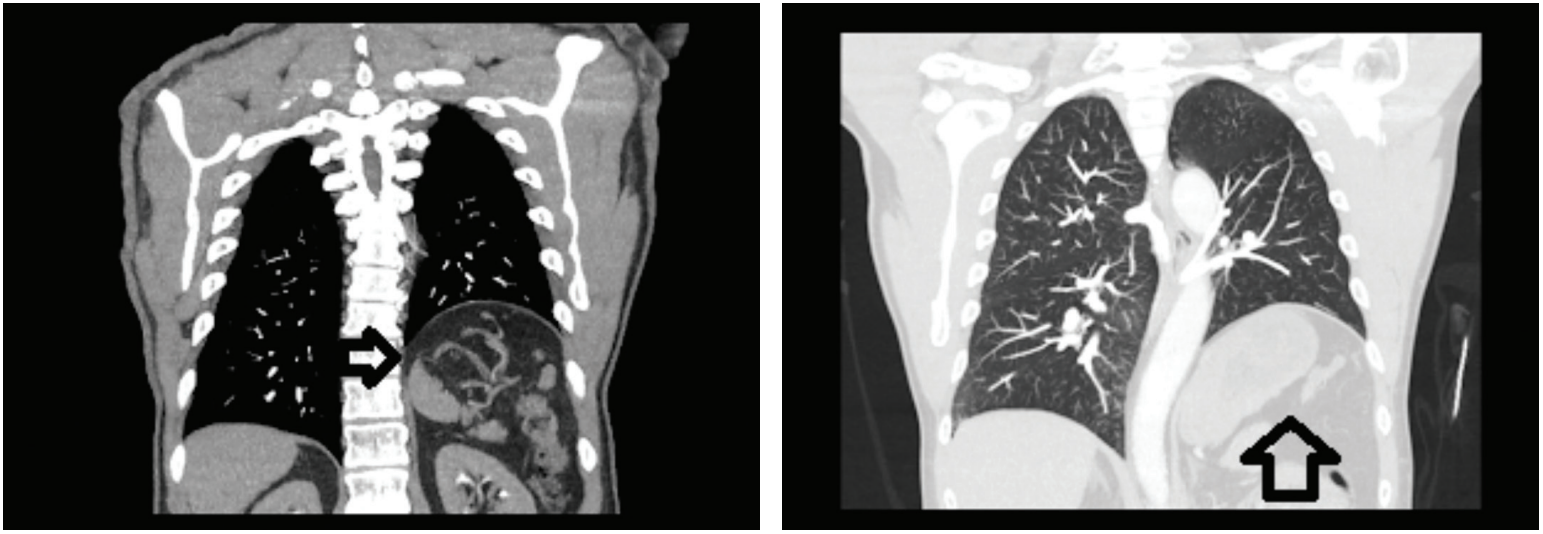
Due to symptoms consistent with unstable angina and a high pretest probability for CAD, a decision was made to take the patient to the cath lab the same day. Left heart catheterization was performed and showed patent coronaries. Prominent elevation of the left diaphragm was seen on multiple cine views with bowel visualization above the heart (Video). Transthoracic echo showed low normal ejection fraction but was otherwise unremarkable. Chest computed tomography (CT) angiography and chest x-ray were negative for pulmonary embolism and showed eventration of the left hemidiaphragm (Figures 1-3).
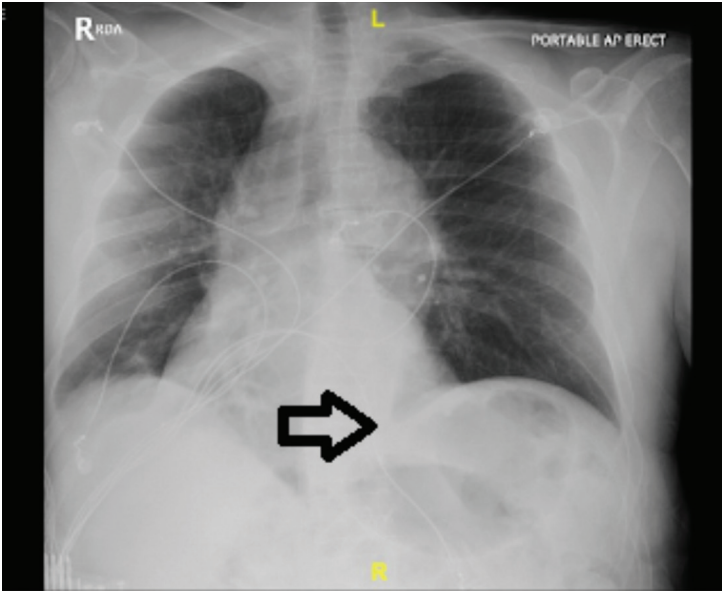
Cardiothoracic surgery was consulted for further evaluation and recommended outpatient follow-up. The patient was discharged in stable condition. He returned the next day with worsening chest pain. Cardiothoracic surgery was reconsulted and left video-assisted thoracoscopic surgery (VATS) with diaphragmatic plication was performed, with resolution of symptoms on follow-up (Figure 4).
Discussion
Diaphragmatic eventration is the abnormal elevation of a part or the whole hemidiaphragm, and can be unilateral or bilateral. It occurs due to lack of muscle or phrenic nerve function. The initial insult leads to a thin and weak diaphragm, resulting in reduced function. Data on incidence is lacking, with the best estimate of around 0.05%. However, the true incidence is higher as most patients are asymptomatic and the condition remains underdiagnosed. It occurs more commonly in men and affects the left hemidiaphragm, as in our patient’s case. Right-sided eventration is less common due to quicker closure of the right pleuroperitoneal hiatus.1-5
Most cases are discovered incidentally, as patients are usually asymptomatic. Other adult patients present with respiratory symptoms, i.e., dyspnea on exertion, orthopnea, tachypnea, recurrent respiratory infections, atelectasis, and chronic cough. Chest pain and arrhythmias may also be present. Gastrointestinal symptoms include dyspepsia, dysphagia, and epigastric pain.6 A chest x-ray and CT imaging are usually done initially.7
Our patient presented with features of worsening severity and frequency of anginal-like pain, with improvement of symptoms after nitroglycerin administration. The etiology of his diaphragmatic eventration was likely a result of trauma from his history of bull riding, with each injury leading to a worsening of the eventration. The improvement of symptoms with sublingual nitroglycerin is possibly due to smooth muscle relaxation including the esophagus, stomach, intestines, and the diaphragm. This likely led to decreased mechanical tension as well as decreased phrenic nerve irritation, and an improvement of symptoms.8
Diaphragmatic eventration can be due to a congenital abnormality or can be acquired. The congenital form is due to incomplete muscularization of the membranous diaphragm. The acquired form is due to trauma, inflammation, or neoplasm.8 Our patient had a history of multiple, traumatic injuries from bull riding and to our knowledge, no other case has been published highlighting this particular etiology. Other imaging modalities, e.g., fluoroscopy and magnetic resonance imaging, are used for diagnosis and surgical planning. Symptomatic patients are treated with diaphragmatic plication with thoracotomy or VATS.3
Conclusion
This case represents acquired diaphragmatic eventration as a rare cause of anginal-like chest pain. It highlights the importance of taking a thorough history and an awareness of local cultural practices, in this case, bull riding. It also illustrates the need to look at non-cardiac findings on cath cines to avoid missing the “elephant in the room.”
References
1. Agarwal AK, Lone NA. Diaphragm Eventration. [Updated 2024 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
2. Guzman JPS, Delos Santos NC, Baltazar EA, Baquir ATD. Congenital unilateral diaphragmatic eventration in an adult: A rare case presentation. Int J Surg Case Rep. 2017; 35: 63-67.
3. Ali Shah SZ, Khan SA, Bilal A, et al. Eventration of diaphragm in adults: eleven years experience. J Ayub Med Coll Abbottabad. 2014 Oct-Dec; 26(4): 459-462.
4. Makwana K, Pendse M. Complete eventration of right hemidiaphragm: A rare presentation. J Family Med Prim Care. 2017 Oct-Dec; 6(4): 870-872.
5. Dahal A, Singh Y, Ansari A, et al. Eventration of diaphragm of unknown cause: a case report. International Journal of Surgery Open. 2023 Aug; 57:100653. https://doi.org/10.1016/j.ijso.2023.100653.
6. Groth SS, Andrade RS. Diaphragm plication for eventration or paralysis: a review of the literature. Ann Thorac Surg. 2010 Jun;89(6):S2146-S2150. doi: 10.1016/j.athoracsur.2010.03.021
7. Midrio P, Gobbi D, Baldo V, Gamba P. Right congenital diaphragmatic hernia: an 18-year experience. J Pediatr Surg. 2007 Mar; 42(3): 517-521. doi:10.1016/j.jpedsurg.2006.10.044
8. Grailey K, Glasziou PP. Diagnostic accuracy of nitroglycerine as a ‘test of treatment’ for cardiac chest pain: a systematic review. Emerg Med J. 2012 Mar; 29(3): 173-176. doi:10.1136/emj.2010.103994
Find More:
Renal Denervation Topic Center
Cardiovascular Ambulatory Surgery Centers (ASCs) Topic Center
Grand Rounds With Morton Kern, MD
Peripheral Artery Disease Topic Center