Eighty Years Undetected: A Congenital Coronary Cameral Fistula Without Significant Shunt
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Abdul Wahab, MD1; Sachin Joseph, MD1; Andres Vargas-Estrada, MD2
1Internal Medicine Residency, FSU College of Medicine, Tallahassee, Florida; 2Interventional Cardiology, Tallahassee Memorial Hospital, Tallahassee, Florida
Disclosures: The authors report no conflicts of interest regarding the content herein.
The authors can be contacted via Sachin Joseph, MD, at sachin.joseph2023@gmail.com
Case
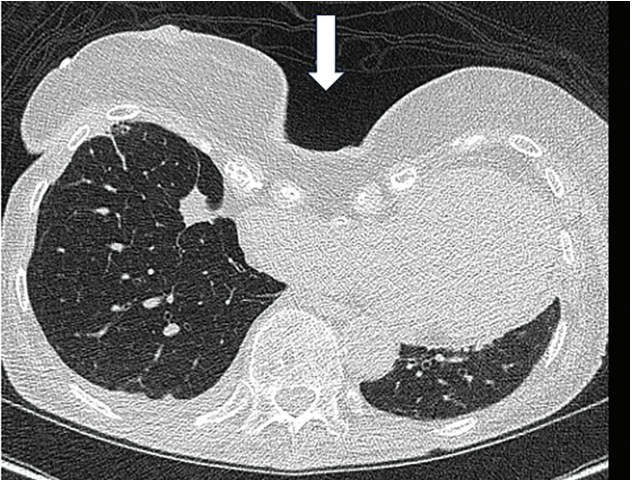
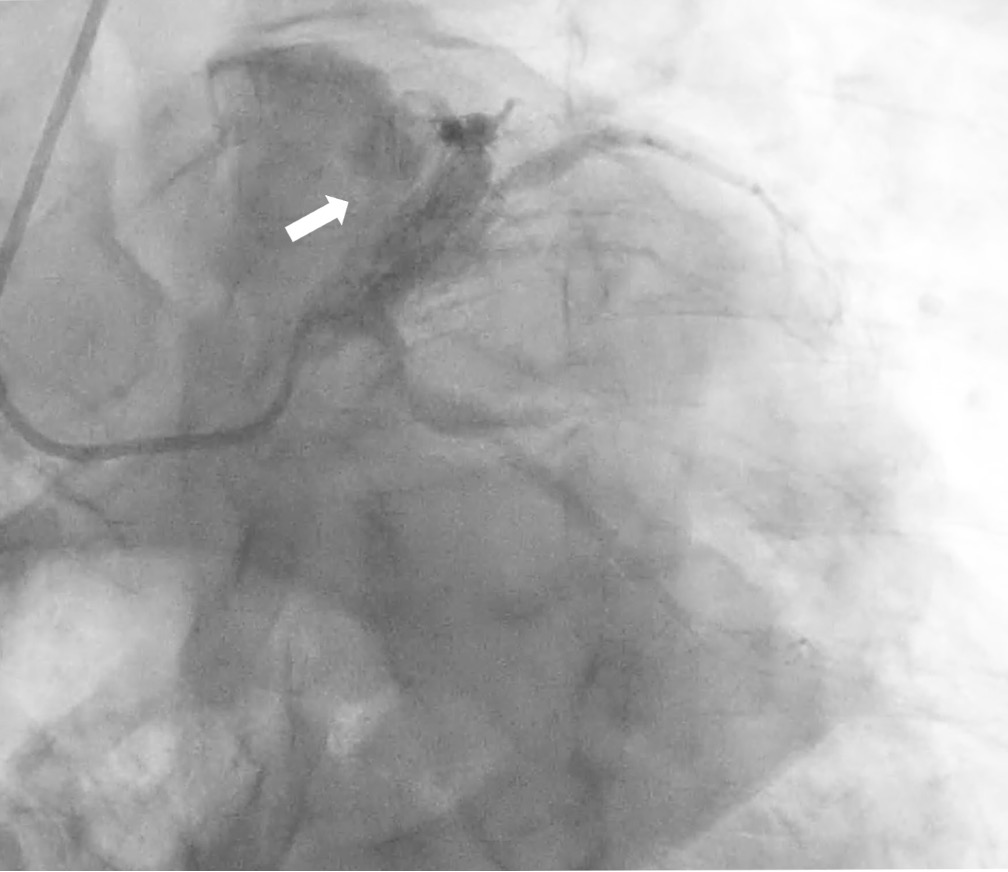
An 80-year-old male with hypertension and hyperlipidemia presented with chest discomfort and dyspnea. Initial investigations, including electrocardiogram and labs, were unremarkable. However, the patient had a high outpatient coronary artery calcium score which prompted further workup. Left heart catheterization showed a large coronary cameral fistula with multiple connections from the proximal left anterior descending artery to the right ventricular outflow tract and main pulmonary artery, with angiographic evidence of coronary steal (Figure 1, arrow). Right heart catheterization showed stable hemodynamics with a Qp:Qs ratio of 1.0 and no significant oxygen saturation step-up, indicating absence of a hemodynamically significant shunt. Given that the patient has lived 80 years with this congenital condition without right atrial or right ventricular enlargement or significant pulmonary hypertension, the decision was made to manage medically with a beta blocker in addition to continuing aspirin and statin. Timely identification and individualized management of coronary cameral fistulae are essential. Percutaneous closure is first-line for accessible, symptomatic fistulas. Conservative management remains appropriate in asymptomatic, hemodynamically insignificant cases, with close imaging and clinical follow-up as per American College of Cardiology guidelines.
Video
Discussion
A coronary cameral fistula is a rare communication between a coronary artery and a cardiac chamber, bypassing the myocardial capillary network. It mostly arises from the right coronary system and rarely drains to the left-sided cardiac chambers.1 It is seen in less than 1% of the population and incidentally seen in ~0.2% of coronary angiographic studies.2 Coronary angiography remains the gold standard for diagnosis, although non-invasive imaging modalities such as computed tomography angiography, cardiac MRI, and echocardiography can provide valuable anatomical detail.
Assessment should include evaluation of the hemodynamic significance of the fistula, including shunt ratio (Qp/Qs), chamber dilation, or evidence of myocardial ischemia. Most coronary cameral fistulae are asymptomatic and, if small, can be managed conservatively with clinical and imaging follow-up.³ However, symptomatic or hemodynamically significant fistulae may warrant intervention. Indications for closure include ischemia, volume overload, arrhythmias, or increased risk of endocarditis. Management options include medical therapy for symptom control (e.g., antianginals), transcatheter closure (preferred if anatomy is suitable, with coils, plugs, and covered stents) or surgical ligation based on the extent of coronary involvement and degree of drainage into its associated cardiac chamber.4,5 Timely diagnosis and individualized management are essential to prevent long-term complications associated with coronary cameral fistulae.
References
1. Padfield GJ. A case of coronary cameral fistula. Eur J Echocardiogr. 2009; 10(5): 718-720. doi:10.1093/ejechocard/jep049
2. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990; 21(1): 28-40. doi:10.1002/ccd.1810210110
3. Boyle S, Jesuthasan LSB, Jenkins C, Challa P, Ranjan S, Dahiya A. Coronary-cameral fistula. Circ Cardiovasc Imaging. 2019; 12(5): e008691. doi:10.1161/CIRCIMAGING.118.008691
4. Armsby LR, Keane JF, Sherwood MC, Forbess JM, Perry SB, Lock JE. Management of coronary artery fistulae. Patient selection and results of transcatheter closure. J Am Coll Cardiol. 2002; 39(6): 1026-1032. doi:10.1016/s0735-1097(02)01742-4
5. Biorck G, Crafoord C. Arteriovenous aneurysm on the pulmonary artery simulating patent ductus arteriosus botalli. Thorax. 1947; 2(2): 65-74. doi:10.1136/thx.2.2.65
Find More:
Renal Denervation Topic Center
Cardiovascular Ambulatory Surgery Centers (ASCs) Topic Center
Grand Rounds With Morton Kern, MD
Peripheral Artery Disease Topic Center
Podcasts: Cath Lab Conversations